Prostate Cancer Focal Therapy as Primary Treatment
Many Gents and their Carers visit our Low/Intermediate Prostate Cancer Group with the intention of using focal therapy to treat their situation. They believe this minimizes treatment and side effects.
AnCan has never been a huge fan of any form of focal therapy. We strongly hold that it is not needed or appropriate for GG1 (Gleason 3+3) men. If elected, it is largely for men with GG2 (G3+4) and on rare occasions GG3 (G4+3).
A major concern with focal therapy is the high rate of recurrence, no matter the type of focal treatment.. Invariably it is over 50%. Since many trials and practitioners treat men with 3+3 disease with some success, the true rate of failure for men with GG2 and GG3 may be considerably higher.
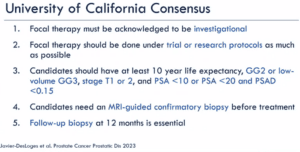
In the UCSF Patient Conference on Prostate Cancer ( April 17, 2026), Dr. Matt Cooperberg presented the following slide that guides AnCan Moderators:
(apologies for clarity… from a screenshot)
Please note AnCan does not provide medical advice. The guidance above is for information only and should be discussed with your medical providers.
Hi-Risk/Recurrent/Advanced PrCa Video Chat, 4/20/26
Survey Opportunity
$200 for a 60min interview. Must be mHSPC or mCRPC; 40-70yr; NOT have used Talzenna, Xtandi or Orgovyx. Reach out to Jason at 773 383 9090 jturner@flinceresearch.com. 15 needed. Indicate you are via AnCan and let us know if accepted (rd@ancan.org)
AnCan thanks the following sponsors for making this recording possible: Novartis, Telix, Blue Earth Diagnostics and Foundation Medicine.
Views expressed in this Recording are solely the opinion of AnCan Foundation, our Moderators and Participants.
AnCan does not accept sponsored promotion. Any drugs, protocols or devices discussed are based solely on anecdotal peer experience or clinical evidence.
AnCan cannot and does not provide medical advice. We encourage you to discuss anything you hear in our sessions with your own medical team.
AnCan reminds all Participants that Adverse Events experienced from prescribed drugs or protocols should be reported to the pharmaceutical manufacturer or the FDA Adverse Event Reporting System (FAERS). To do so call 1-800-332-1066 or download interactive FDA Form 3500 https://www.fda.gov/media/76299/download
All AnCan’s groups are free and drop-in … join us in person sometime! You can find out more about our 12 monthly prostate cancer meetings at https://ancan.org/prostate-cancer/ Sign up to receive a weekly Reminder/Newsletter for this Group or others at https://ancan.org/contact-us/
Join our other free and drop in groups:
Men (Only) Speaking Freely…1st & 3rd Thursdays @ 8.00 pm Eastern https://ancan.org/men-speaking-freely/
Veterans Healthcare Navigation… 1st & 3rd Tuesdays @ 8.00 pm Eastern Schmier Room https://ancan.org/veterans/
Veterans Speaking freely… 4th Tuesday @ @ 8.00 pm Eastern Schmier Room
Editor’s Pick: What to do when assigned control arm in a trial
Topics Discussed
Germline BRCA2 Gent graduates to this group 6 mo. post surgery; heart issues arise – at 87! Can E2 worsen cardiac condition?; entering “Long Game’ trial but wants a GU MO; assigned control in Xalirutamig trial, and seeking alternatives – MSKCC 2nd opinion; embarking on IHT, but very low pulse requires investigation; why’s he getting a PSMA with undetectable PSA – new GU MO could be in order; PSMA and PSA stable – time to debulk?; change HT to daro one year out?; ongoing fatigue – try Wellbutrin; accepted to Long Game, but PSA doubling fast; recurrent Mx Gent finds he’s germline BRCA2 on AnCan’s pushing
AnCan thanks the following sponsors for making this recording possible: Novartis, Telix, Blue Earth Diagnostics and Foundation Medicine.
Views expressed in this Recording are solely the opinion of AnCan Foundation, our Moderators and Participants.
AnCan does not accept sponsored promotion. Any drugs, protocols or devices discussed are based solely on anecdotal peer experience or clinical evidence.
AnCan cannot and does not provide medical advice. We encourage you to discuss anything you hear in our sessions with your own medical team.
AnCan reminds all Participants that Adverse Events experienced from prescribed drugs or protocols should be reported to the pharmaceutical manufacturer or the FDA Adverse Event Reporting System (FAERS). To do so call 1-800-332-1066 or download interactive FDA Form 3500 https://www.fda.gov/media/76299/download
All AnCan’s groups are free and drop-in … join us in person sometime! You can find out more about our 12 monthly prostate cancer meetings at https://ancan.org/prostate-cancer/ Sign up to receive a weekly Reminder/Newsletter for this Group or others at https://ancan.org/contact-us/
Join our other free and drop in groups:
Men (Only) Speaking Freely…1st & 3rd Thursdays @ 8.00 pm Eastern https://ancan.org/men-speaking-freely/
Veterans Healthcare Navigation… 1st & 3rd Tuesdays @ 8.00 pm Eastern Schmier Room https://ancan.org/veterans/
Veterans Speaking freely… 4th Tuesday @ @ 8.00 pm Eastern Schmier Room
Editor’s Pick: Don’t blame it on the prostate cancer… two Gents report tenderness but is it something else?
Topics Discussed
Newbie prescribed singlet HT when doublet was SoC – don’t switch w.3 months left but change docs; is cystoscopy the right procedure?; IHT after 3 years – but what bout shortness of breath; is tenderness from exercise or cancer?; is HT the right first step on BCR; insurance declines Axumin; starting AMG509 xaluritamig trial; stable on mono daro at 86; just finished 6th Pluvicto for foamy cell PrCa; don’t fret over tiny PSA moves; is chest tenderness down to HT or a previous cancer?; not eligible for Capitello trial – needs 2nd opinion on intensification
Chat
AnCan – Ric sent: 3:04 PM
GoTo Help 877 582 7011
Danny sent: 3:13 PM
Have to duck out for a couple of minutes.
David D Seattle sent: 3:14 PM
David joined by phone, I have an update
Len sent: 3:31 PM
Yes, my brother in arms, I was at the beach today. Water temp was 73. Re: your email – did you complete your chest RT?
Hello Steve! Yes, I’ll need to step up my sunblock to spf 50. UV index is high every day. How’s by you?
Adrian (Tony) Bruno sent: 3:51 PM
ask him what his hemoglobin level is
Steve Roux, Up North, Michigan sent: 4:00 PM
I got to run gang. So good to see you all. Great meeting as usual!
Joseph (Sean) Siry – Laguna Woods, CA. sent: 4:04 PM
Dinner is on the table, so I will have to go also– & I can report next time the good news.
AnCan – Rick sent: 4:06 PM
For everyone – Please tell us if you think you need to leave early…(should have added, “and you asked for time’:rd)
Bob Y — Los Angeles sent: 4:13 PM
I also need to leave early. Happy to see all of you.
Jim E., Ft. Worth T sent: 4:17 PM
While I haven’t had “Germline” testing, I had a complimentary gene testing through a group called Color, and they indicated no concerns for increased risk. I have logged in and opened my biopsy and PSMA PET results.
Bruce Schrimpf sent: 4:27 PM
I may have b e to leave there is a tornado warning for areas just to the South of my home. BDS
AnCan thanks the following sponsors for making this recording possible: Novartis, Telix, Blue Earth Diagnostics and Foundation Medicine.
Views expressed in this Recording are solely the opinion of AnCan Foundation, our Moderators and Participants.
AnCan does not accept sponsored promotion. Any drugs, protocols or devices discussed are based solely on anecdotal peer experience or clinical evidence.
AnCan cannot and does not provide medical advice. We encourage you to discuss anything you hear in our sessions with your own medical team.
AnCan reminds all Participants that Adverse Events experienced from prescribed drugs or protocols should be reported to the pharmaceutical manufacturer or the FDA Adverse Event Reporting System (FAERS). To do so call 1-800-332-1066 or download interactive FDA Form 3500 https://www.fda.gov/media/76299/download
All AnCan’s groups are free and drop-in … join us in person sometime! You can find out more about our 12 monthly prostate cancer meetings at https://ancan.org/prostate-cancer/ Sign up to receive a weekly Reminder/Newsletter for this Group or others at https://ancan.org/contact-us/
Join our other free and drop in groups:
Men (Only) Speaking Freely…1st & 3rd Thursdays @ 8.00 pm Eastern https://ancan.org/men-speaking-freely/
Veterans Healthcare Navigation… 1st & 3rd Tuesdays @ 8.00 pm Eastern Schmier Room https://ancan.org/veterans/
Veterans Speaking freely… 4th Tuesday @ @ 8.00 pm Eastern Schmier Room
Editor’s Pick: Dr. Kwon… either overtreating or undertreating! And… Crestor & Nubeqa don’t mix!
Topics Discussed
Repeat recurrences since 2019 may be down to shorter periods of HT; Gent pushes for Axumin and gets it; should he debulk?; add back E2; is Kwon overtreating with triplet? – get thee to a GU med onc; stable but needs a new GU med onc – or does he?; HT is doing exactly what it should; doing well on mono daro but needs help with back pain; rosuvastatin doesn’t play well with daro; numbers good after stopping HT but fatigue/weakness persists; RT requires self catheterizing; fatigue/weakness could be recent covid; experience with PCPEP
Chat
Alfredo in Wimberley sent: 5:24 PM
UW-OncoPlex™ is a multiplexed mutation assay for tumor tissue that assesses mutations >400 genes related to cancer treatment, prognosis, or diagnosis (listed below). UW-OncoPlex™ is intended for solid tumors.
Sorry Fellas, I need to leave early. I will pose my question next week. Thanks!
“Thomas” M Vancouver,WA sent: 6:45 PM
Pregabalin (Lyrica)
Jim Marshall, Vet Support Grp. Moderator sent: 6:48 PM
Might want to look at PRAVASTATIN as an alternative. I could not handle Crestor or Lipitor. Jim Marshall
Bruce Schrimpf sent: 6:52 PM
The worst thing about a colonoscopy is the prep not the procedure itself. During the procedure you’re in La-la Land!
Jeff Marchi – San Francisco sent: 6:53 PM
exactly
Bruce Schrimpf sent: 6:54 PM
Indeed!
Jeff Marchi – San Francisco sent: 6:55 PM
👍
david opp sent: 6:56 PM
I am going to call it a night, I will try for next Tuesday.
Peter M sent: 7:05 PM
Great meeting! Good night!
“Thomas” M Vancouver,WA sent: 7:07 PM
Excuse me, gents. Leaving the meeting. Thanks to all.
Pierre D., Olean NY sent: 7:14 PM
I joined PC-PEP a week ago and find it helpful.
Bruce Schrimpf sent: 7:15 PM
I had COVID during the time I was on Lupron. I was retired so I took noon time naps. I believe in the less medication the better! It makes me feel better and improves my bank account!
Joseph (Sean) Siry – Laguna Woods, CA. sent: 7:17 PM
Have a healthy week
Bruce Schrimpf sent: 7:18 PM
Always good seeing and hearing all of you. Good night (Guten Nacht Auf Deutsch). BDS
AnCan thanks the following sponsors for making this recording possible: Novartis, Telix, Blue Earth Diagnostics and Foundation Medicine.
Views expressed in this Recording are solely the opinion of AnCan Foundation, our Moderators and Participants.
AnCan does not accept sponsored promotion. Any drugs, protocols or devices discussed are based solely on anecdotal peer experience or clinical evidence.
AnCan cannot and does not provide medical advice. We encourage you to discuss anything you hear in our sessions with your own medical team.
AnCan reminds all Participants that Adverse Events experienced from prescribed drugs or protocols should be reported to the pharmaceutical manufacturer or the FDA Adverse Event Reporting System (FAERS). To do so call 1-800-332-1066 or download interactive FDA Form 3500 https://www.fda.gov/media/76299/download
All AnCan’s groups are free and drop-in … join us in person sometime! You can find out more about our 12 monthly prostate cancer meetings at https://ancan.org/prostate-cancer/ Sign up to receive a weekly Reminder/Newsletter for this Group or others at https://ancan.org/contact-us/
Join our other free and drop in groups:
Men (Only) Speaking Freely…1st & 3rd Thursdays @ 8.00 pm Eastern https://ancan.org/men-speaking-freely/
Veterans Healthcare Navigation… 1st & 3rd Tuesdays @ 8.00 pm Eastern Schmier Room https://ancan.org/veterans/
Veterans Speaking freely… 4th Tuesday @ @ 8.00 pm Eastern Schmier Room
Editor’s Pick: addressing insomnia… and AnCan helps men switch docs.
Topics Discussed
T3b Gent needs clarification on his Bx before starting treatment; how much HT before discussing intermittent; starting doublet; Nagar suggests IMRT is better for this Gent; switching HT drugs may address castrate resistance; Cialis for nocturia – maybe; potential cardio-onc in Portland, OR; Kishan’s ANDROMEDA trial attractive to men with slow recurrence; can prostate cancer cells be dormant?… follow up post-recording suggests YES.