
Rarity Life Magazine Featuring Rick Davis
Rarity Life Magazine Feature: Rick Davis
AnCan’s ambitious CEO and Founder, Rick Davis, recently sat down with Rarity Life, the magazine published by Same But Different Creative, to share the deeply personal journey that led to the creation of AnCan.
In the interview, Rick reflects on his early days navigating a prostate cancer diagnosis — a moment that reshaped his life & his understanding of what true support should look like. Like so many survivors and thrivers, he quickly discovered that information alone isn’t enough. What people often need most is connection — the chance to speak openly with others who truly understand the lived experience of cancer.
That realization became the foundation of AnCan.
Rick shares how traditional support models don’t always meet people where they are. Geographic limitations, physical health challenges, financial strain, rare diagnoses, and even the emotional weight of walking into an in-person group can all create barriers. For many, simply showing up can feel overwhelming.
AnCan was built to remove as many of those barriers as possible.
Rick’s full interview in Rarity Life offers an inspiring look at leadership shaped by lived experience, and a reminder that meaningful change often begins with one person asking: How can we do this better?
Read more stories & Rick’s article here:
https://www.samebutdifferentcic.org.uk/raritylife
AnCan GU ASCO26 survivorship poster: participants strongly endorse our Groups

AnCan GU ASCO26 survivorship poster: participants strongly endorse our Groups
For release on Monday, Feb 23, 2026
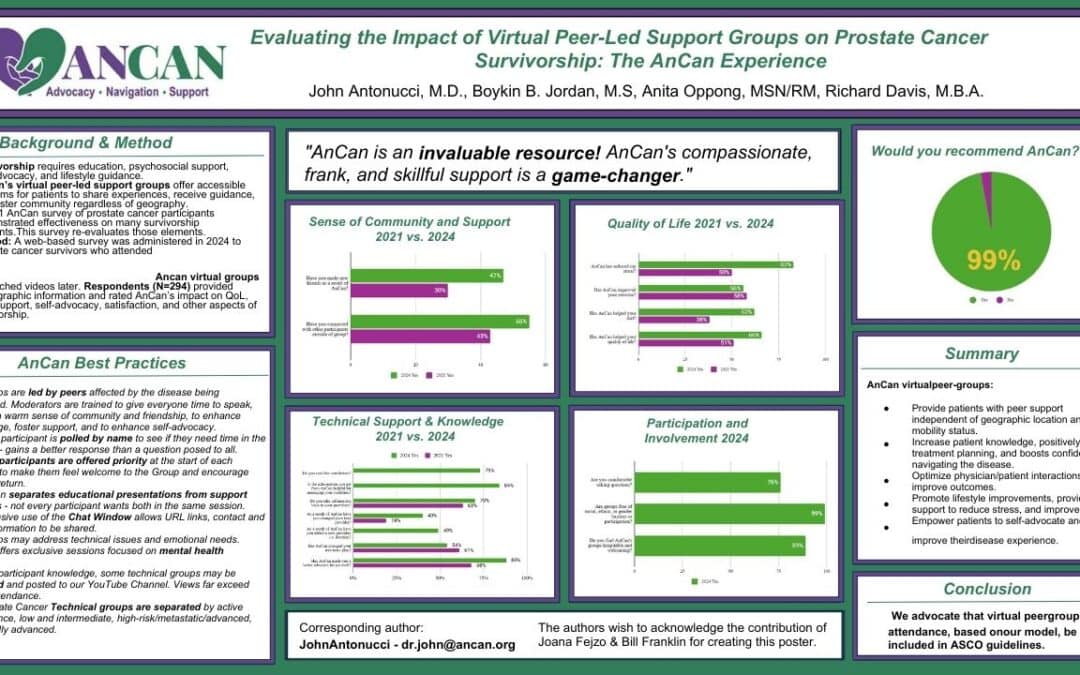
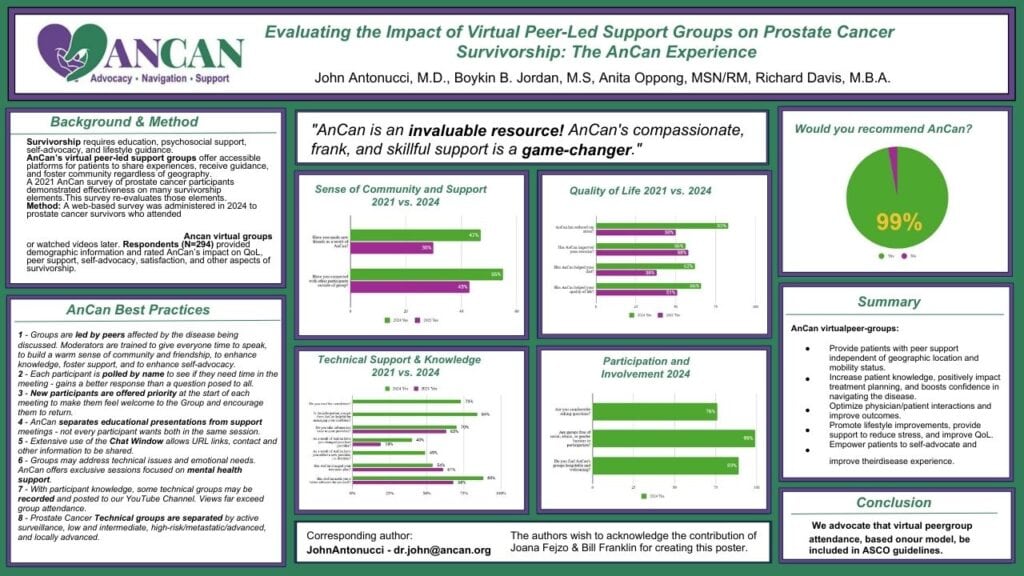
AnCan Foundation strongly believes we run the best support groups available!! We can now release the first results of our 2024 AnCan Participant Survey that confirms that our participants think so too. This first batch of results is taken from almost 300 prostate cancer responses at all levels of disease.
- 99% of respondents would recommend AnCan Groups
- 66% improved Quality of Life – 83% noted reduced stress; 62% improved nutrition; 56% increased exercise
- 88% advocated better for themselves and AnCan influenced over half (54%) the treatment paths
- 47% made new friendships – AnCan’s personal favorite since this extends support well beyond our Groups
If you’re attending GU ASCO26 , please stop by our poster on Friday, Feb 27 to meet Dr. John Antonucci, discuss these astonishing results and the AnCan method, and pick up a flyer of the poster.
CONTACT
- Dr. John Antonucci dr.john@ancan.org 262 264 8011
- Rick Davis rd@ancan.org 262 264 8011


ABSTRACT
Evaluating the impact of virtual peer-led support groups on prostate cancer survivorship: the AnCan experience.
John Antonucci*, Boykin B. Jordan, Anita Oppong, Richard Davis
- Abstract Number: 265
- Poster Board Number: A23
- Session Title: Poster Session B: Prostate Cancer and Urothelial Carcinoma
- Date and Time: February 27, 2026, 11:30 AM-12:45 PM; 4:45 PM-5:45 PM (PST)
Background: Comprehensive prostate cancer (PCa) survivorship requires more than just clinical care, including education, psychosocial support, self-advocacy, and lifestyle guidance—needs often unmet by traditional oncology visits. Virtual peer-led support groups, such as those offered by the AnCan Foundation, offer accessible, real-time platforms for patients to share experiences, receive guidance, and foster community, regardless of geography. This study evaluates the impact of AnCan participation on factors known to be associated with a better quality of life (QOL) among PCa survivors.
Methods: A web-based survey was administered in 2024 to PCa survivors who attended or expressed interest in AnCan meetings. Respondents (N=294) provided demographic information and rated AnCan’s impact on QOL, peer support, self-advocacy, and satisfaction. Data were analyzed to assess the subjective influence of AnCan’s virtual support model on survivorship.
Results: (2021 results are in brackets for comparison.) Most respondents were in their 60s–70s (75%), highly educated (82%), and 55% had incomes over $100,000. Eighty-three percent had someone in their lives they could rely on and with whom they maintained regular contact.
Nearly all (97%) found AnCan meetings helpful for disease understanding, learning options, and well-being. Sixty-six percent reported improved QOL; 83% [50%] noted reduced stress; 62% [38%] improved nutrition; and 56% [58%] increased exercise. Satisfaction was high, with 99% recommending AnCan.
AnCan involvement enhanced self-advocacy (88%), improved patient-provider communication, and improved decision-making. Seventy percent brought information from AnCan to their providers, 49% added new providers, and 40% changed their lead provider. Over half (54%) reported that AnCan influenced their treatment path.
Socially, 55% [43%] connected with peers outside meetings, and 47% made new friendships.
Conclusions: Survey responses indicate that the AnCan virtual peer-led model, to be described in the poster, meaningfully increases patient knowledge, empowers self-advocacy, reduces stress, and fosters healthy behaviors, improving quality of life for PCa survivors. We advocate for integrating such peer support into NCCN, AUA, and ASCO survivorship guidelines.
POSTER
CNTV’s “Best of the Nation” featuring Rick Davis
CNTV’s “Best of the Nation” featuring Rick Davis
CNTV’s recent video features an interview with AnCan founder, Rick Davis. He explains that he started AnCan after his own diagnosis in 2007, after realizing inadequate support options, especially for those in remote areas. AnCan aims to eliminate barriers to entry for its various support groups, which range from cancer to chronic diseases. AnCan empowers patients to “Be your own best advocate” by providing them with the knowledge to speak confidently with their healthcare providers and offering peer-to-peer support.
Spirituality Improves your Health!
Written by: Dr. John Antonucci
As we always emphasize, taking care of our hearts (the actual organ) is very important to us PCa guys. For metastatic men, a very substantial minority of us will die of heart disease before our PCa gets us. For non-metastatic, more than half will.
So when Rick saw an article about the Cardiology Society of Sao Paulo devoting a seminar to Spirituality in the treatment of heart disease, he sent it right over to me with a suggestion to make it an invitation. The cardiologists reported that there are spiritual factors that benefit cardiovascular health, reduce cardiac hospitalizations, lower blood pressure, and even improve survival.
The “spiritual” factors the Sao Paulo group discussed are things like purpose in life, gratitude, hope, and “moral, emotional, and mental values that shape an individual’s behavior and decision-making.”
“Spirituality cuts across and transcends a person’s life, shaping their choices and way of living.” There are scales to measure spirituality for research purposes.* High scores on these scales correlate with the “depth of spirituality” with less hypertension, better cardiac output, better compliance with treatments, lower levels of fight-or-flight nervous activity, lower stress hormones, less inflammation, fewer hospitalizations, less anger, less anxiety, and longer life. Actual heart attacks are linked to acute stress, and spirituality helps lower that risk.
Treatment for spiritual distress has been tried. In one study, videos about spiritual reflection, gratitude, forgiveness, life purpose, and optimism produced drops in BP and better blood vessel endothelial function.
Since there is an overlap between “spirituality” and “religiosity”, several studies have separated the two, and the benefits described above do not extend to “religious” practices like attendance at services, religious rituals, or structured participation in a religion.
It is the same for cancer; research shows that spirituality plays a significant role in cancer. Spirituality practices made their way into Palliative Care Medicine years ago, particularly in end-of-life care and acceptance. “Spiritual distress,” however defined, is very common in cancer patients. And patients believe that their healthcare providers should consider their spiritual needs, and that this is often not done.
Let’s look in the NCCN and ASCO** cancer treatment guidelines for the word “spirituality”:
NCCN now has a “distress management” section where they recommend screening for distress, including spiritual concerns, as part of routine oncology care. If spiritual or existential concerns are found, they encourage referral to chaplains, spiritual counselors, or mental health professionals trained in spiritual issues. NCCN states that spirituality practices can improve quality of life, coping strategies, and treatment adherence.
ASCO also calls for psycho-social screening in oncologic care, which should encompass spiritual health. They advocate addressing spiritual concerns as an integral part of supportive care, and encourage open communication about spiritual and existential concerns, respecting patient preferences and cultural backgrounds.
Neither group provides detailed protocols for spirituality practices like they do for, say, chemotherapy, but both call for the integration of spiritual assessment and support in cancer care. They acknowledge that addressing spiritual needs can improve emotional well-being, coping, and overall quality of life for cancer patients.
We in MSF are wary of discussing religion. However, both cardiology and oncology sources separate religion from spirituality. It seems we should tactfully inquire about this together, since it is correlated with cardiac and oncologic outcomes and quality of life.
*We don’t have to use other folks’ definitions of spirituality, but here are a few of the assessments you can try out:
- ONC-5 chaplain assessment of explicit spiritual concerns in cancer patients: https://www.youtube.com/watch?v=hhlJKPsBSqE
- FICA spiritual assessment tool: https://coalitionccc.org/CCCC/CCCC/Resources/FICA-Spiritual-Assessment-Tool.aspx
- https://spiritualityandhealth.duke.edu/files/2024/11/fitchett-new-approaches-to-sp-assess-112624-002.pdf
**The National Comprehensive Cancer Network and the American Society of Clinical Oncology.

Dr. John Antonucci on “Grief”
Dr. John Antonucci on “Grief”
“Someone I once loved gave me a box of darkness” –Mary Oliver
I was at a 12-Step-oriented workshop about grief recently, and it made me think about Men Speaking Freely (MSF). We are vaguely aware of grief in all MSF groups, it hangs over us, and we have at times focused on some specific griefs/losses, such as vitality, or a longer life. It is commonly thought that not thinking about a loss, not talking about it is the manly thing to do. Here in MSF we get relief by sharing our common losses with each other.
The presenter of that workshop, Marcia C., had some ways to specifically talk about grief that were new to me. She gave me permission to use some of her material here. She pointed out some types of losses that I hadn’t realized. For example, the loss of who I would have been if cancer didn’t happen, the grief of estrangement, loss of work, of status, of friendship; the loss of never having had something, that of aging, of trust, or of giving up something.
She said there is “unacknowledged grief” when such losses are never fully brought to consciousness. When I looked at her long list of examples I saw many that I have. We ought to watch for unacknowledged grief.
She described “non-finite” grief, which has no end-point other than death. Ours could be in that category, since as time goes by our loss increases instead of lessens.
Marcia said, ‘’Sharing your grief is a way to receive validation and compassionate witnessing. It can help you begin a path to healing and/or finding a way to live with grief.
Consider the questions below:
1. Are there griefs you haven’t realized you have or have been afraid to face?
2. Are there griefs about which you’d like to share?
3. Do you have grief practices that might be helpful to others?
4. Make a list of griefs you’ve experienced.
5. Choose a tool from the list that might help you process your grief.”
That list of “tools” was long; it included things like: write a letter or poem describing our loss…Create a ritual of letting go…Share with others who have had similar losses…Visit a place that is meaningful…Make or buy a talisman that helps you feel protected…Dance, run, yell to get your feelings out of your body…Plant something in remembrance or as a new beginning…Start a new tradition…Do an intentional funeral… These are ways to bring acknowledged, unacknowledged, and non-finite grief out for a conscious conversation. Moving from covert to overt, with the goal of making a relationship with the loss, and getting rid of the unconscious silent prolonged scream that I, for example, think I harbor.
We think of grief as emotional, but in “Dealing With the Physical Impact of Intense Grief” by Batya Swift Yasgur, the author describes the variety of physical reactions to grief. Ranging from elevated blood pressure to takotsubo cardiomyopathy — sometimes called “broken heart syndrome” — which is a “stress response that balloons the heart.” We often wonder about the reaction on our immune system, and its implications to our overall survival. In fact, probably nearly all our systems react to grief in some way.
There is a fairly new grief-related diagnosis in the Diagnostic and Statistical Manual and the International Classification of Diseases, describing a “persistent and pervasive grief response” that goes on longer than a year., and is now called Prolonged Grief Disorder. In order to be diagnosed with Prolonged Grief Disorder, a person must experience at least three of eight additional symptoms that include “disbelief, intense emotional pain, feeling of identity confusion, avoidance of reminders of the loss, feelings of numbness, intense loneliness, meaninglessness, or difficulty engaging in ongoing life” according to Columbia University’s Center for Prolonged Grief. For an adult to meet the criteria for a PGD diagnosis, the death of a loved one must have occurred at least one year ago, and the symptoms must be present most days since the loss and nearly every day for at least the last month.
Our situation is different from losing a loved one (although it includes that) and waiting for the grief to go away. Instead of a major loss which goes farther and farther into the past, our major loss is in the future. We have sort of a reverse Prolonged Grief Disorder. For instance, I expect my losses to get worse and worse until death.
November 1, 2023