Living with cancer often means living with uncertainty, and for many patients, that uncertainty shows up as fear of recurrence and the very real stress of upcoming scans, tests, and follow-up appointments. In his introduction for the most recent Men Speaking Freely on June 4th, Dr. John provides a great summary of the Fear of Cancer Recurrence:
I thought I’d take a new look at a favorite topic of ours, Fear of Recurrence. Here is an update from recent literature.
Not that we need a definition, but FCR is defined in the literature as the fear, worry, or concern that cancer will return or progress. It’s among the most common and persistent concerns for cancer survivors, including men with prostate cancer. It seriously affects our quality of life, mental health, and even relationships.
Recent studies confirm that at least half of cancer survivors experience moderate to high FCR, with 10–20% experiencing severe, disabling FCR. Younger age, female gender, recent diagnosis, low social support, poor physical condition, and previous psychological difficulties are risk factors for higher FCR in general. For prostate cancer, younger patients and those with PSA increases or ambiguous test results are at higher risk. Of course, men may underreport FCR due to stigma or stoicism (fancy word for being stupid).
Cognitive Behavioral Therapy (CBT) and Mindfulness-Based Interventions are still the most evidence-based approaches. New trials support the efficacy of both in reducing FCR, including when delivered via telehealth.
Structured interventions like ConquerFear (iConquerFear) and SWORD (Survivors’ Worry Reduction) are scientifically validated in multiple countries and are worth looking at. There’s supposed to be an Australian intervention called iCanADAPT for prostate cancer, but I can’t seem to navigate to it from icandapt.adaptcancer.org.au. Meta-analyses show modest benefit for these interventions, with high patient acceptability.
Medications addressing fear of recurrence are still not supported as primary treatment, but they sure got me by those early months without adverse effects.
The International Psycho-Oncology Society and ASCO survivorship guidelines, as well as recent research, recommend regular assessment and referral for FCR. Tools like the Fear of Cancer Recurrence Inventory (FCRI), FCR-7, and Cancer Worry Scale are available, but I’ve never heard of anyone being screened. Wake up, docs.
On the horizon, studies are examining genetics, inflammation, and personality traits as predictors of FCR. Interventions are becoming culture-specific.
So, FCR is normal, and severe/persistent FCR is treatable. Routine discussion and screening for FCR should be part of survivorship care. Effective interventions (CBT, mindfulness, research-based web-based programs) are available and increasingly accessible. Patients should not hesitate to raise FCR concerns – help is available.
-Dr. John Antonucci MD
With thanks to one of our own, Andy Douglas, a recent webinar from Smilow Cancer Hospital at Yale, part of its Survivorship Series, goes into far more detail and is worth watching. In Unraveling Fear of Cancer Recurrence: Realities and Tools for Coping (https://www.youtube.com/watch?v=27aHVlFsgN4), presenters Gabriel Cartagena, PhD, Angela Khairallah, MSW, LCSW, and Susanne Lee-Baldassini, LCSW, examine fear of cancer recurrence and “scanxiety,” explaining how common these experiences are and offering practical coping strategies for managing them.
Not everyone will experience fear of cancer recurrence or scan-related anxiety in the same way, but these concerns are common across the cancer community. This webinar will not make uncertainty disappear, but it does offer grounded, practical tools that can help patients and families navigate it with more confidence. If you’re struggling with anxiety, read the recent Substack post by Howard Hertz: Anxiety and the Miscalibrated Mind. Hertz breaks down how our brains are evolutionarily hard-wired to prioritize survival over factual accuracy, meaning your brain would rather make the mistake of feeling anxious than risk being caught off guard.
A relatively new year, new guidelines, and new tools for prostate cancer screening and monitoring.
In recent months, the AUA updated its 2023 guidelines specifically for early detection of prostate cancer (https://www.auanet.org/guidelines-and-quality/guidelines/early-detection-of-prostate-cancer-guideline). Along with those guidelines, two other organizations have updated or developed additional tools that are beneficial to all men, regardless of where they are on the prostate cancer journey (or even those not yet on a journey).
Consider them collectively as an introduction to screening (NCCN), an AS-focused source (ASPI), and a comprehensive guide for early-stage prostate cancer.
I would not consider any of them as a standalone product for all the information a man might need. The NCCN guidelines are focused on screening and are relatively basic. ASPI’s product is focused on AS, but some may find the scope and scale of information a bit overwhelming without someone to advise and assist them. The appendix at the end of the pamphlet would be exceedingly useful for anyone beginning their prostate cancer journey. Finally, the AUA guidelines are broader and developed more for urologists.
Learn from AnCan’s Emperors of Estradiol… video chat and discussion
AnCan would bet no other prostate cancer support group has the experience and knowledge around using estradiol.
For those unfamiliar, estradiol is a female hormone that is found in men in small part; just like women carry a low level of testosterone (T). In large levels, estradiol (E2) can suppress T and effectively do the work of androgen deprivation, without many of the side effects of ADT. It is cheap and effective and has been around many years. So cheap that many pharmaceutical companies are concerned it can replace a primary, far more profitable ADT agent… like Lupron, Eligard, Firmagon or Orgovyx. Robert Reich, former Secretary of Labor, makes the argument better than I can.
It offers a much higher Quality of Life, and the recent PATCH trial has shown its efficacy and non inferiority. The major disadvantages are 1) getting a doctor to prescribe it since it is not FDA approved and must be prescribed off label. And 2) gynecomastia (breast enlargement) that can be painful and socially embarrassing, although it has remedies.
Two of the most outspoken and well recognized advocates for E2 are peer users associated with AnCan. Dr. Paul Schellhammer, a former President of the American Urological Association, is on our Brains Trust. Dr. Richard Wassersug is on AnCan’s Advisory Board. Both have used E2 for more than 20 years, while AnCan member Al Latimer outlasts them both – but not together.
Listen to this outstanding discussion… yet again AnCan’s information is PRICELESS!
AnCan’s ambitious CEO and Founder, Rick Davis, recently sat down with Rarity Life, the magazine published by Same But Different Creative, to share the deeply personal journey that led to the creation of AnCan.
In the interview, Rick reflects on his early days navigating a prostate cancer diagnosis — a moment that reshaped his life & his understanding of what true support should look like. Like so many survivors and thrivers, he quickly discovered that information alone isn’t enough. What people often need most is connection — the chance to speak openly with others who truly understand the lived experience of cancer.
That realization became the foundation of AnCan.
Rick shares how traditional support models don’t always meet people where they are. Geographic limitations, physical health challenges, financial strain, rare diagnoses, and even the emotional weight of walking into an in-person group can all create barriers. For many, simply showing up can feel overwhelming.
AnCan was built to remove as many of those barriers as possible.
Rick’s full interview in Rarity Life offers an inspiring look at leadership shaped by lived experience, and a reminder that meaningful change often begins with one person asking: How can we do this better?
AnCan GU ASCO26 survivorship poster: participants strongly endorse our Groups
For release on Monday, Feb 23, 2026
AnCan Foundation strongly believes we run the best support groups available!! We can now release the first results of our 2024 AnCan Participant Survey that confirms that our participants think so too. This first batch of results is taken from almost 300 prostate cancer responses at all levels of disease.
99% of respondents would recommend AnCan Groups
66% improved Quality of Life – 83% noted reduced stress; 62% improved nutrition; 56% increased exercise
88% advocated better for themselves and AnCan influenced over half (54%) the treatment paths
47% made new friendships – AnCan’s personal favorite since this extends support well beyond our Groups
If you’re attending GU ASCO26 , please stop by our poster on Friday, Feb 27 to meet Dr. John Antonucci, discuss these astonishing results and the AnCan method, and pick up a flyer of the poster.
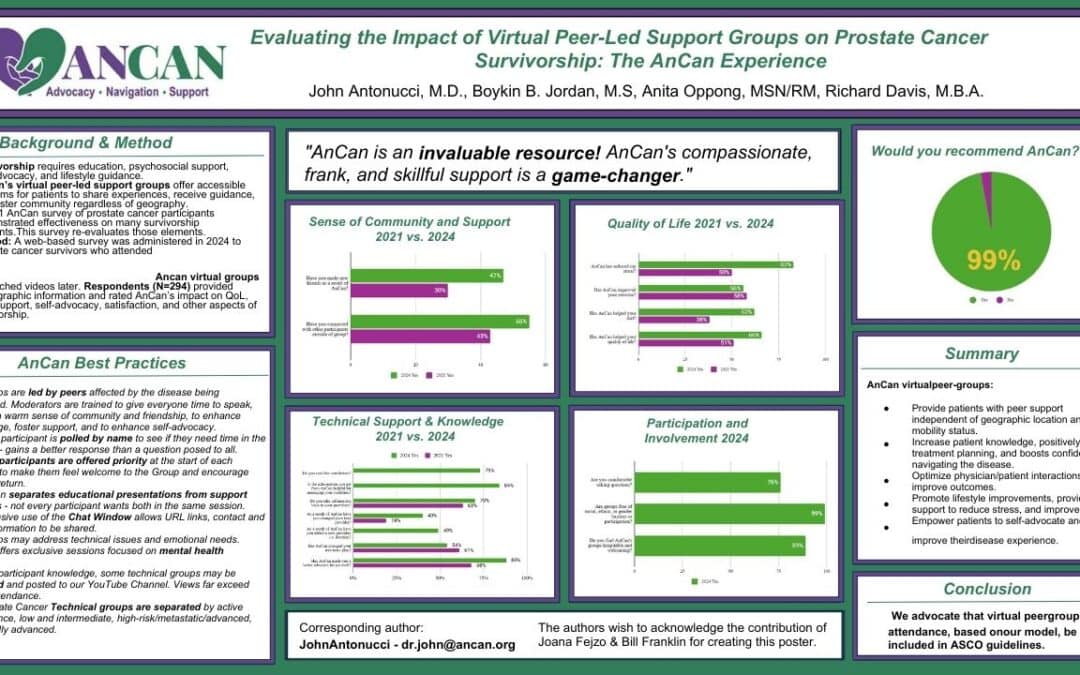
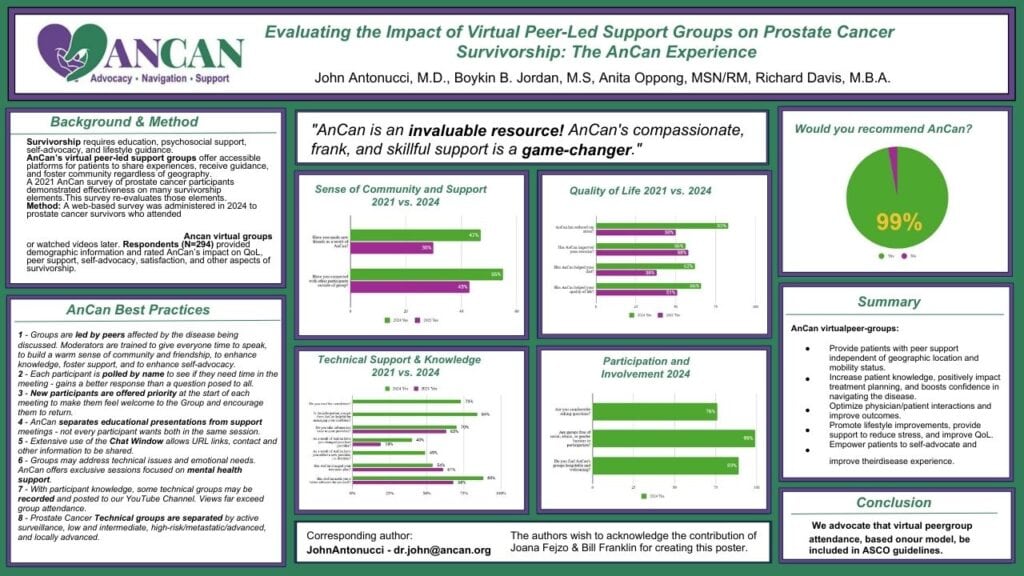
Evaluating the impact of virtual peer-led support groups on prostate cancer survivorship: the AnCan experience.
John Antonucci*, Boykin B. Jordan, Anita Oppong, Richard Davis
Abstract Number: 265
Poster Board Number: A23
Session Title: Poster Session B: Prostate Cancer and Urothelial Carcinoma
Date and Time: February 27, 2026, 11:30 AM-12:45 PM; 4:45 PM-5:45 PM (PST)
Background: Comprehensive prostate cancer (PCa) survivorship requires more than just clinical care, including education, psychosocial support, self-advocacy, and lifestyle guidance—needs often unmet by traditional oncology visits. Virtual peer-led support groups, such as those offered by the AnCan Foundation, offer accessible, real-time platforms for patients to share experiences, receive guidance, and foster community, regardless of geography. This study evaluates the impact of AnCan participation on factors known to be associated with a better quality of life (QOL) among PCa survivors.
Methods: A web-based survey was administered in 2024 to PCa survivors who attended or expressed interest in AnCan meetings. Respondents (N=294) provided demographic information and rated AnCan’s impact on QOL, peer support, self-advocacy, and satisfaction. Data were analyzed to assess the subjective influence of AnCan’s virtual support model on survivorship.
Results: (2021 results are in brackets for comparison.) Most respondents were in their 60s–70s (75%), highly educated (82%), and 55% had incomes over $100,000. Eighty-three percent had someone in their lives they could rely on and with whom they maintained regular contact.
Nearly all (97%) found AnCan meetings helpful for disease understanding, learning options, and well-being. Sixty-six percent reported improved QOL; 83% [50%] noted reduced stress; 62% [38%] improved nutrition; and 56% [58%] increased exercise. Satisfaction was high, with 99% recommending AnCan.
AnCan involvement enhanced self-advocacy (88%), improved patient-provider communication, and improved decision-making. Seventy percent brought information from AnCan to their providers, 49% added new providers, and 40% changed their lead provider. Over half (54%) reported that AnCan influenced their treatment path.
Socially, 55% [43%] connected with peers outside meetings, and 47% made new friendships.
Conclusions: Survey responses indicate that the AnCan virtual peer-led model, to be described in the poster, meaningfully increases patient knowledge, empowers self-advocacy, reduces stress, and fosters healthy behaviors, improving quality of life for PCa survivors. We advocate for integrating such peer support into NCCN, AUA, and ASCO survivorship guidelines.
As some of you may know, the liberal telehealth rules to conduct medical appointments remotely that were enabled during Covid, sunsetted late last year. AnCan was upset and vocal that many of our patient advocacy organizations active on The Hill did not campaign more widely to extend it. Organizations like ZERO (prostate cancer) have significant and expensive government relations groups precisely to address such issues on behalf of us patients. AnCan had to bring it to ZERO’s attention to move the ball at a time when ZERO’s high paid CEO was self-admittedly sleeping on the switch.
Telehealth was temporarily extended for those living in rural areas. Then one of our newly minted prostate cancer Moderators, David Sharpe, brought it to AnCan’s attention that legislation was passed on Feb 3, 2026 that has extended comprehensive telehealth through the end of 2027. We asked David to blog its welcome return to wider availability and tell his story around telehealth – thank you Mr. Sharpe!
Medicare Telehealth Coverage Is Extended
The federal government has restored Medicare coverage for telehealth until the end of 2027. That means you can now possibly consult with your doctors online rather than having to meet with them in-person.
Why did I say possibly? Because state medical licensing laws still apply. Often, they can undermine your doctor’s ability to join you on the call. Here’s why: (Don’t construe the following comments as legal or medical advice. This is general information only.)
Telehealth consultations are easiest to arrange when a patient and doctor are in the same state. For instance, if you live in Springfield, Illinois, and want to have a virtual chat with an oncologist in Chicago, no legal impediments are likely to stand in your way.
Things can get tougher if the doctor practices in another state. Physicians are typically required to be licensed in the state where the patient is physically located during the consult. Therein lies a common problem: the doctor is licensed in one state, and you’re in another.
But loopholes exist. According to the Center for Connected Health Policy (CCHP), “A few states have licenses or telehealth-specific exceptions that allow an out-of-state provider to render services via telemedicine in a state where they are not located, or allow a clinician to provide services via telehealth in a state if certain conditions are met (such as agreeing that they will not open an office in that state). Still other states have laws that don’t specifically address telehealth and/or telemedicine licensing, but make allowances for practicing in contiguous states. . . .” For specifics about your state’s rules, explore CCHP’s handy state-by-state guide: https://www.cchpca.org/topic/cross-state-licensing-professional-requirements/.
Despite those exceptions, many physicians and medical centers require patients to be in the same state as the doctor during telehealth appointments. I wish I’d known that last year, before trying to set up virtual consultations from my home in Portland, Oregon, with Fred Hutch (Washington), UCSF, City of Hope (both California), and MD Anderson (Texas0—all of whom turned me down. Oregon Health & Science University (OHSU, Oregon)) would have refused, too, if I had been in any other state.
But some physicians and hospitals were more relaxed about it. Despite remaining in Portland, I wrangled a telehealth visit with a UCLA specialist. Two AnCan buddies of mine in Oregon and Arizona did so as well. I had even better luck with out-of-state doctors in community practices. Two agreed to confer with me online, and one declined.
If you live near—but not in—the state where your doctor practices, perhaps the easiest option is to make a run for the border. One AnCan member has adopted that strategy as a convenient means of communicating with his faraway medical team in an adjacent state while also satisfying the legal requirements. To have that meeting, he travels a few miles from home to a casino just across the state line; the casino lets him conduct telehealth consultations there. That approach shaves hours off what would otherwise be a protracted road trip to talk with his doctors face-to-face. # # #