Has eating become a challenge due to fatigue or a lack of interest in food? Have you noticed a significant change in your or your loved one’s appearance since starting treatment or diagnosis?
It’s a common misconception that weight loss during cancer treatment is solely due to treatment side effects. While this can certainly be a factor, a more serious condition known as cachexia (kuh·kek·see·uh) can significantly impact a patient’s health.
What is Cachexia and Who is at Risk?
Cachexia, often referred to as cancer cachexia or wasting syndrome, is a complex condition characterized by severe weight loss, muscle wasting, and loss of appetite. It’s not a direct side effect of cancer treatment but rather a consequence of the cancer itself. While it’s commonly associated with cancer, it’s important to note that cachexia can affect individuals with various chronic illnesses, including: Multiple Sclerosis, Sarcoidosis, heart failure, chronic kidney disease, COPD, and more. Certain types of cancer are more likely to lead to cachexia than others. These include: Pancreatic, Lung, Head and Neck, Colorectal, Ovarian, and Liver.
Signs and Symptoms of Cachexia: What Should You Look For?
Recognizing the signs of cachexia is crucial for early intervention and effective management. Here are some key symptoms to watch for:
Unexplained weight loss: A significant and unintentional decrease in weight.
Muscle loss: A noticeable loss of muscle mass, often leading to weakness and fatigue.
Decreased appetite: A reduced desire to eat, even when hungry.
Fatigue: Persistent tiredness and a lack of energy.
Metabolic changes: Alterations in metabolism, including changes in appetite, weight, and energy levels.
Changes in Routine: Unable to do the activities you once could.
If you or a loved one is experiencing these symptoms, it’s important to let your care team know your concerns as soon as possible.
Managing Cachexia
While there’s no one-size-fits-all solution, a multidisciplinary approach can help manage the condition. This may involve:
Dietary interventions: A registered dietitian can provide personalized meal plans to maximize nutrient intake.
Medical treatments: In some cases, medications may be prescribed to stimulate appetite or reduce inflammation.
Supportive care: This includes strategies to manage pain, fatigue, and other symptoms.
Psychological support: Counseling can help address emotional challenges associated with cachexia.
This may mean adding more people to your careteam to support you, such as a dietician (as shown above), physical or occupational therapist, endocrinologist, or palliative care (editors note: we hope you already have a palliative care doctor, AnCan loves them and they can offer you so much support during your treatment!)
Coping with the Emotional Impact
Cachexia can take a significant toll on both physical and emotional well-being for the patient, care-partner, and their families. It’s important to seek support to manage the emotional side effects of the condition. Consider:
Counseling: Individual, couples, or family therapy can provide guidance and coping strategies.
You can also ask your social worker (or for a social worker if you do not have one) for additional resources.
Want to Learn More?
We highly recommend this webpage and fact sheet from our friends at Cancer Support Community / Gilda’s Club. While it is cancer centric, all of the information will be of helpful no matter what your diagnosis is.
By understanding the complexities of cachexia and seeking appropriate support, individuals can significantly improve their quality of life. Effective management of cachexia can help alleviate debilitating symptoms, enhance overall well-being, and improve the ability to participate in daily activities.
Special thanks to CSC for their assistance and incredible resources with this blog post.
Birdability: Accessibility and Inclusiveness in The Outdoors
If you’ve ever been to one of the AnCan art classes, you might know me as the art/ painting instructor. It’s me, hi! I’m the kind of person who likes to make it my business to remind everyone to take a deep breath and smell the roses. Maybe paint the roses, too. Do something you love to do. That’s easy to say to an able-bodied person. What if you’re not quite an able-bodied person, but you still adore outdoor activities, like bird-watching?
That’s where Birdability comes into the picture! Meet Virginia Rose; Birdability’s Founder and Chair Emeritus. Virginia fell off a horse when she was a teenager, and has been a wheelchair user ever since. She and Rick Davis had a chance encounter at the grocery store recently when he helped her reach a bottle of champagne from the shelves. That’s where he learned all about Birdability and Virginia’s passion for merging accessibility with her love for birds and natural spaces.
Birdability works hard to call attention to the need for accessible spaces and an inclusive mindset in places that aren’t traditionally thought of as accessible: the outdoors.
“Often it is the environment that is disabling, rather than the person who is disabled” – Birdbility
Their entire mission is to bring the joys of birding and the outdoors to those who may not otherwise be able to experience it. Birding was a hobby that Virginia really leaned into and it helped her to “discover her best self in nature”. Birding can be for anybody and and body; it’s up to the abled to be welcoming to those who may not be as abled.
Even if you, or a friend, have some visual impairments, there are guides on how to bird watch with limited vision; including using sounds and tools to help with your identification. Maybe some of our VSS people can benefit?
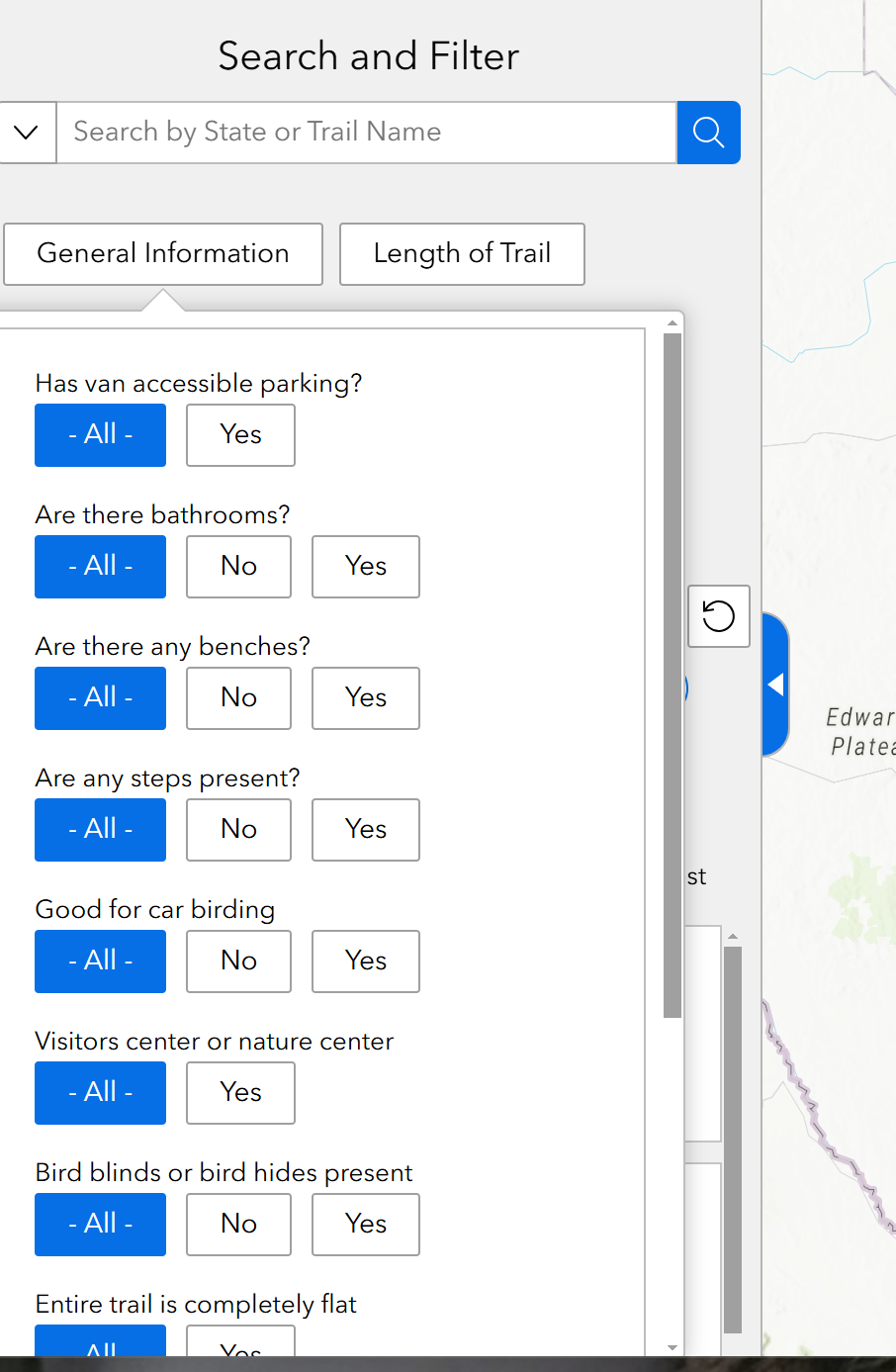
Probably my favorite feature, however, has to be the birding map, which was made in partnership with the National Audubon Society and local contributors. It’s a map intended to help locate accessible trails and outdoor spaces throughout the world. You can filter through so many different features, including surface type (asphalt, concrete, gravel, etc), bathrooms along a trail, parking fees, car birding, and so much more.
I scrolled through other continents just to see what’s out there. I’m sad (but not surprised) to see that there’s not much in he way of accessibility outside the United States, Canada, and Europe. I’m sure there are more parks and places that can be added. I think this just shows how much of a necessary resource that this organization provides. Honestly, I may even use this tool myself to find accessible trails for my own outdoor activities, like painting outside in the park.
“Websites and recommendations from park staff are frequently incomplete — and so unreliable — sources of a location’s true accessibility, and what is accessible for one user may not be accessible for another.”
So many of us want to be outside, but just can’t find reliable information about how to just exist outside. It’s easy to say that an outdoor area has accessible pavement, for example, but is the concrete well-managed and actually accessible for a wheelchair or cane user? Is it on a slope? Are there van-accessible parking spaces? Is there enough shade from the sun? Are there food trucks or other snack/food options? So many things to consider.
That’s where you, if you’re interested in birding, can come in and organize a fun local meetup. You have the tools you need right here!
Anyway, hopefully it isn’t too cold for you to be outside just yet! Go check out Birdability and their Blog and tell us what you think!
Hi-Risk/Recurrent/Advanced PCa Video Chat, Dec 2, 2024
HAVE YOU COMPLETED THE ANCAN SURVEY???
If you clicked on this recording and the answer is NO, please ask yourself why not?! We do a lot for you – take 7 minutes right now to complete our AnCan participant survey for us and for you. https://docs.google.com/forms/d/e/1FA… . If YES – thank YOU!!
AnCan is grateful to the following sponsors for making this recording possible: Bayer, Foundation Medicine, Janssen, Myriad Genetics, Novartis, Telix & Blue Earth Diagnostics.
AnCan’s Annual Fundraiser is nigh – we only bother you once a year. Not even an email on Giving Tuesday! PLEASE support us generously – pharma sponsorship is down this year and AnCan needs grassroots participants to compensate. Please treat us generously. https://ancan.org/donate/
AnCan respectfully notes that it does not accept sponsored promotion. Any drugs, protocols or devices recommended in our discussions are based solely on anecdotal peer experience or clinical evidence.
AnCan cannot and does not provide medical advice. We encourage you to discuss anything you hear in our sessions with your own medical team.
AnCan reminds all Participants that Adverse Events experienced from prescribed drugs or protocols should be reported to the pharmaceutical manufacturer or the FDA Adverse Event Reporting System (FAERS). To do so call 1-800-332-1066 or download interactive FDA Form 3500 https://www.fda.gov/media/76299/download
All AnCan’s groups are free and drop-in … join us in person sometime!
Editor’s Pick: Gents compare ‘holiday’ notes. And maybe heart muscle is compromised by ADT (rd)
Topics Discussed
Newbie joins us in time for his holiday; whatever happened to ‘triplet’ therapy for high volume denovo Mx Gent; spot RT starts, daro stops and more chemo; one opinion suggests HT holiday now – is that smart?; his holiday has been good – can it continue?; don’t knock yourself out with KP/NIH when you have VA and Tricare for Life; wassup with Medicare Telehealth in 2025?; ‘Cushingoid’ moon face suggests time to drop steroids + abi.
AnCan is grateful to the following sponsors for making this recording possible: Bayer, Foundation Medicine, Janssen, Myriad Genetics, Novartis, Telix & Blue Earth Diagnostics.
AnCan respectfully notes that it does not accept sponsored promotion. Any drugs, protocols or devices recommended in our discussions are based solely on anecdotal peer experience or clinical evidence.
AnCan cannot and does not provide medical advice. We encourage you to discuss anything you hear in our sessions with your own medical team.
AnCan reminds all Participants that Adverse Events experienced from prescribed drugs or protocols should be reported to the pharmaceutical manufacturer or the FDA Adverse Event Reporting System (FAERS). To do so call 1-800-332-1066 or download interactive FDA Form 3500 https://www.fda.gov/media/76299/download
AnCan’s Prostate Cancer Forum is back (https://ancan.org/forums). If you’d like to comment on anything you see in our Recordings or read in our Reminders, just sign up and go right ahead. You can also click on the Forum icon at the top right of the webpage.
All AnCan’s groups are free and drop-in … join us in person sometime!
Editor’s Pick: He starts forgetting words in mid-sentence — is it his ADT? (bn)
Topics Discussed
Reminder to complete the AnCan survey — this includes those who watch our recordings!; entering “the most intense time of my 5 1/2 years with prostate cancer” as cancer recurs and chemo and bone radiation begin; 550 genes in his report — but not many will be actionable; close relatives have prostate cancer, but nothing shows on germline tests — perhaps it was a toxic exposure?; a colon cancer gene mutation is found to be driving his prostate cancer — does he have both?; bizarre insurance company denial has him scratching his head; don’t let VA paperwork stand in the way of a PSMA PET; platelet clumping in his blood tests isn’t likely to be disease-related; he starts forgetting words midsentence — is ADT to blame?; his doc restarts the ADT clock — this time with standard-of-care intensification; why CT and bone scan, but no PSMA PET?; doctors don’t talk to each other anymore, and patient care suffers.
Chat Log
Jim Marshall, Alexandria, VA · 6:36 PM
TCEs are known causes of Prostate. Cancer. Jim
AnCan – rick · 6:46 PM
MUTYH is the driver mutation that Joel had
AnCan – rick · 6:50 PM
Pesticides adn Prostate Cancer https://acsjournals.onlinelibrary.wiley.com/doi/abs/10.1002/cncr.35572?mc_cid=c1825f551a&mc_eid=838454d636
Jerry G, Brighton, MI · 7:19 PM
estradiol helps
Steve Roux, North Michigan · 7:24 PM
thanks! I’ll ask Dr. Fedak.
Steve L · 7:54 PM
Thanks to all. Happy Thanksgiving!
Steve L · 8:01 PM
Orca in photo was taken from my boat .
Julian – Houston · 8:08 PM
Happy Thanksgiving to ALL!!!
Steve Roux, North Michigan · 8:09 PM
This group empowers us to be our own best advocate.
J. Ward · 8:09 PM
Thankful for AnCan. Happy Thanksgiving, everyone!
Steve Roux, North Michigan · 8:10 PM
I need to sign off…..Tucker the rescue pup and my wife require my attention. HAVE AN AWESOME THANKSGIVING DAY!
Why Your Practice Should Join the Veterans Administration (VA) Community Care Network
The health and well-being of Veterans are of the utmost importance, and community healthcare providers play a vital role in ensuring they receive the timely and high-quality care they deserve. The VA Community Care Network (CCN) bridges the gap between Veterans and community practices, offering an invaluable opportunity for providers to expand their impact while supporting those who served.
What is the VA Community Care Network (CCN)?
The VA CCN is a program established under the VA MISSION Act of 2018 to ensure that Veterans can access care outside of VA facilities when it is in their best interest. Whether a Veteran lives too far from a VA medical center or needs a service not available within the VA, the CCN provides them access to a broad network of community-based healthcare providers.
By partnering with the VA, community practices gain the ability to treat Veterans while ensuring seamless coordiation of care, referrals, and reimbursement. It should be noted the program is structured to reimburse the providers at a MEDICARE Reimbursement rate for any scheduled procedure or service, and the two payers who manage the program have kept a record of repayments within 30 days of proper billing. Through their contracts with the VA, they have been incentivized properly to ensure providers are properly reimbursed for the valuable service provided.
Why Should Your Practice Join the CCN?
Serve Those Who Served Us
Veterans have made sacrifices for our country, and healthcare providers have the chance to give back by ensuring they receive the care they need, closer to home.
Many Veterans face barriers to accessing VA facilities due to location, schooling, capacity, or specific care requirements. By joining the CCN, your practice can play a critical role in removing these barriers.
Expand Your Patient Base
Participation in the CCN opens the door to a steady stream of patients referred by the VA, providing stability and opportunities for growth in your practice.
Veterans represent a large and diverse group of patients with a variety of healthcare needs, from routine check-ups to specialized treatments.
Streamlined Reimbursement
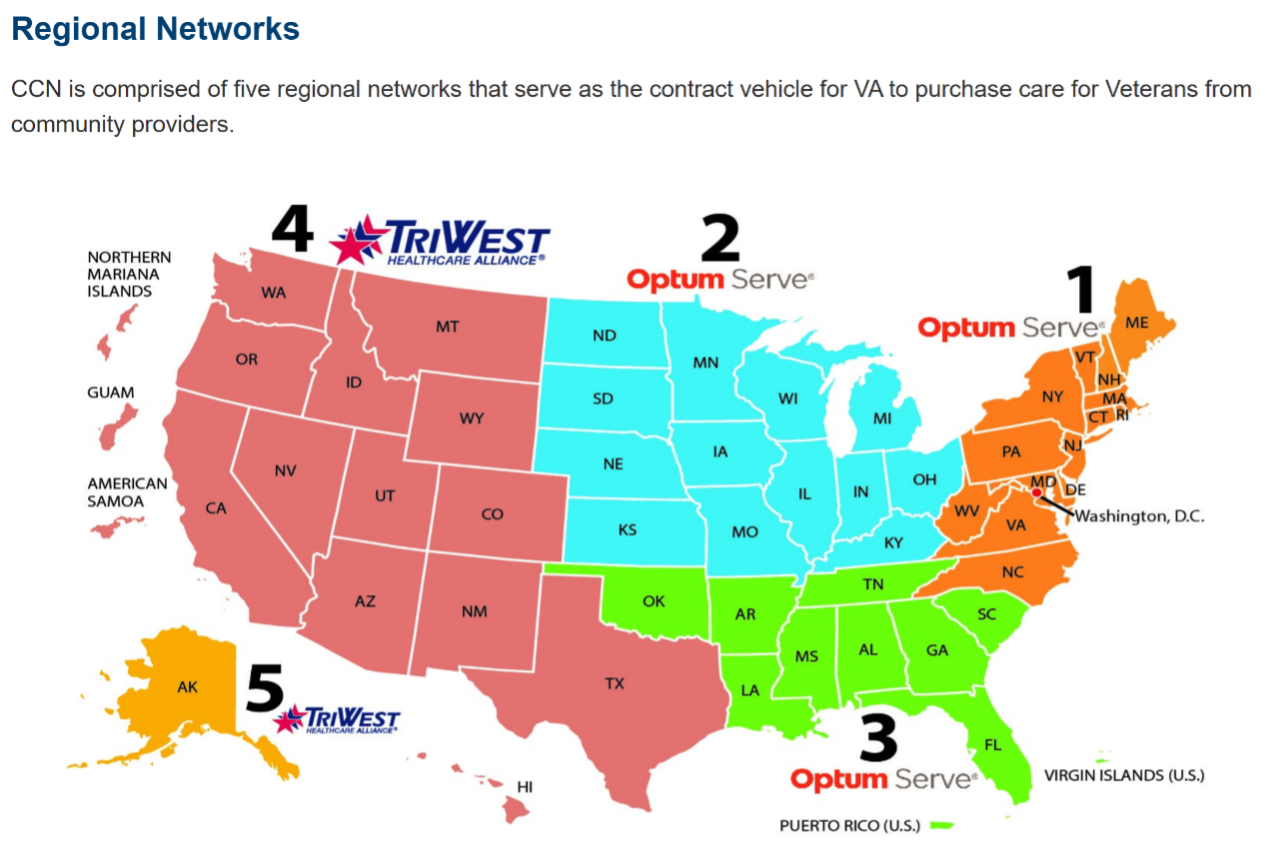
The VA CCN ensures that providers are reimbursed for the care they deliver through its partnership with regional administrators like Optum and TriWest.
By meeting CCN requirements, your practice can enjoy smooth billing processes and prompt payment for services rendered.
Improve Veteran Health Outcomes
Veterans often face unique health challenges, such as higher rates of certain chronic illnesses and service-related conditions. As a CCN provider, you can contribute to improving their quality of life through timely, high-quality care.
Simplified Enrollment Process
Joining the CNN is straightforward. Practices need to determine their region, ensure they meet Medicare reimbursement standards, and establish a Veterans Care Agreement (VCA). Once enrolled, your practice will be equipped to provide care to Veterans in your area.
How to Join the VA Community Care Network
Determine your region (Regions 1-3 are managed by Optum, and Regions 4-5 are managed by TriWest.)
Contact the appropriate regional adminsitrator to initiate the enrollment process:
Optum Regions (1-3): Call 800-901-7407 or visit their provider page.
https://vacommunitycare.com/provider
TricWest Regions (4-5): Call 1-855-722-2838 or visit their provider page.
https://www.triwest.com/en/veteran-services/
Review requirements for a Veterans Care Agreement (VCA) and complete your enrollment.
A Veteran’s Journey Through CCN
A Veteran seeks care through their VA provider.
The VA determines the Veteran qualifies for community care and refers them to an in-network provider.
The community provider delivers care and submits medical records back to the VA.
The provider bills Optum or TriWest for reimbursement.
By joining the CCN, your practice becomes an essential part of this seamless process, ensuring Veterans get the care they deserve.
Conclusion
Joining the VA Community Care Network is more than a business opportunity—it’s a chance to make a meaningful difference in the lives of Veterans. By enrolling, your practice can contribute to a healthier future for those who served while benefitting from increased patient volume and streamlined processes.
Take the next step today and learn how your practice can make a difference.
By : Mike “Bing” Crosby, Veterans Prostate Cancer Awareness Inc, mike.crosby@vpca.vet
Ancan would like your input on its future planning and academic research. Please take a few minutes to complete The 2024 AnCan Survey which is at thislink.
AnCan is grateful to the following sponsors for making this recording possible: Bayer, Foundation Medicine, Janssen, Myriad Genetics, Novartis, Telix & Blue Earth Diagnostics.
WELCOME all to our newly recorded Low/Intermediate Prostate Cancer Group. To receive notice when new recordings are posted, either follow us on this YouTube Channel or sign up to our Blog via https://ancan.org/contact-us/ – check New Blog box.
AnCan respectfully notes that it does not accept sponsored promotion. Any drugs, protocols or devices recommended in our discussions are based solely on anecdotal peer experience or clinical evidence.
AnCan cannot and does not provide medical advice. We encourage you to discuss anything you hear in our sessions with your own medical team.
AnCan reminds all Participants that Adverse Events experienced from prescribed drugs or protocols should be reported to the pharmaceutical manufacturer or the FDA Adverse Event Reporting System (FAERS). To do so call 1-800-332-1066 or download interactive FDA Form 3500 https://www.fda.gov/media/76299/download
AnCan’s Prostate Cancer Forum is back (https://ancan.org/forums). If you’d like to comment on anything you see in our Recordings or read in our Reminders, just sign up and go right ahead. You can also click on the Forum icon at the top right of the webpage.
All AnCan’s groups are free and drop-in … join us in person sometime!
Editor’s Pick: Focal therapy delays the time for more definitive treatment options. (bj)
Topics Discussed
Long-term treatment options for post radiation urinary issues; learn the importance of getting a second opinion on a prostate biopsy – active surveillance may be an option. Getting a Decipher test — testing to determine the liklihood of cancer spreading; Prostate Cancer Research Institute (PCRI) is a valuable information source; Additional tests to screen for prostate cancer, such as: EpiSwitch PSE and ExoDx Prostate Test; Considering focal treatment options with a cribriform pattern and intraductal indications — High-Dose (HDR) Brachytherapy, High Intensity Focal Ultrasound (HIFU) and Tulsa-PRO; Prostox DNA testing to determine risk for Genitourinary (GU) toxicity.
Chat Log
AnCan – rick
unauthorized!!!
Tim in Tampa
I completed the survey yesterday!
AnCan – rick
Tx Tim….
AnCan – rick
Ming Zhou https://profiles.mountsinai.org/ming-zhou
AnCan – rick
JH 2nd opinion https://pathology.jhu.edu/patient-care/second-opinions
Causley
Boykin is the star. He is the guru with this matter.
AnCan is grateful to the following sponsors for making this recording possible: Bayer, Foundation Medicine, Janssen, Myriad Genetics, Novartis, Telix & Blue Earth Diagnostics.
AnCan respectfully notes that it does not accept sponsored promotion. Any drugs, protocols or devices recommended in our discussions are based solely on anecdotal peer experience or clinical evidence.
AnCan cannot and does not provide medical advice. We encourage you to discuss anything you hear in our sessions with your own medical team.
AnCan reminds all Participants that Adverse Events experienced from prescribed drugs or protocols should be reported to the pharmaceutical manufacturer or the FDA Adverse Event Reporting System (FAERS). To do so call 1-800-332-1066 or download interactive FDA Form 3500 https://www.fda.gov/media/76299/download
AnCan’s Prostate Cancer Forum is back (https://ancan.org/forums). If you’d like to comment on anything you see in our Recordings or read in our Reminders, just sign up and go right ahead. You can also click on the Forum icon at the top right of the webpage.
All AnCan’s groups are free and drop-in … join us in person sometime!
Editor’s Pick: Don’t use a PA or NP to make treatment decisions; closely followed by – audit your medical records! (rd)
Topics Discussed
Deferring treatment on recurrence ain’t a great idea; newbie needs MSKCC referral and we personally endorse two docs; check your medical records – you might find something that never happened; exercise recs for man with heart issues; PROMISE shows no mutations; Payer forces switch of RT provider at last minute; here’s why you avoid a PA or NP if a treatment decision is next; does cribriform change treatment?; value of AI retrospective opinion – even if available; treatment veteran moves to Jevtana; why genetic counseling before germline test; abi-enz sequencing discussion
If any of you new people are Veterans, contact me at CaptJim@AnCan.Org Jim Marshall, USAF(Ret)
Luther
sent: 6:59 PM
enjoyed tonight’s Meeting and will register at conclusion of meeting
Adam
sent: 7:01 PM
Definitely wasn’t covering your ass. Thanks for another great session guys. I have to check out. Survey done!
John A
sent: 7:08 PM
thanks Adam
Steve Roux, North Michigan
sent: 7:10 PM
I visit my patient portal after every office/lab visit. There is a note at the top of the page to contact them if there are any errors. I have done that in the past to correct notes from my 1st med onc.
AnCan – rick
sent: 7:14 PM
Max heart rate – 220 minus age
Alfredo in Houston
sent: 7:16 PM
Steve, all the organizations that care for my wife and I use the same Electronic Medical Record, and they are able to share test results as well with our permission. We pay attention to our After Visit Summaries after every contact. Unfortunately, this is not true for all patients all over the USA
Julian – Houston
sent: 7:21 PM
have to leave early – Great discussion
Alfredo in Houston
sent: 7:30 PM
Agree with everything Rick just said! Unfortunately I have to go. Thanks to all y’all; See you next time.
Steve Roux, North Michigan
sent: 7:39 PM
hey guys – great meeting – I gotta run tho. See you next week!
Thomas M
sent: 8:06 PM
See you all next time, gents. Thanks.
Jim Marshall, Alexandria, VA
sent: 8:07 PM
Jim Marshall. 703-338-7341. CaptJim@rickd13.sg-host.com Veterans
100% Free VA Healthcare Entitlement per the TERA Memo
For all Vietnam, Gulf War, Middle East and Southwest Asia veterans covered under the PACT Act of 2022, you are now entitled to FREE VA Healthcare with the exposure to toxic materials because of TERA (Toxic Exposure Risk Activity). Sep 20, 2023 — In August 2022, the PACT Act was signed and expanded benefits and services for veterans with toxic exposures during service. Even if you have a VA Disability rated at 10%-40% or never, ever applied for any VA Disability Rating, the veteran is now eligible for free healthcare.
A TERA memorandum, or toxic exposure risk activity report, is a document that the VA medical examiner reviews when a veteran files a disability claim that references the PACT Act. The PACT Act, or Honoring our PACT Act of 2022, expanded benefits and services for veterans who were exposed to toxins while serving in the military.
Presently VA FREE Healthcare is available for those who:
CATEGORY 1: Veterans who participated in a toxic exposure risk activity (as defined by law) while serving on active duty, active duty for training, or inactive duty training.
Note: many stateside & overseas military posts and bases have been declared Toxic Waste Sites. These are not automatic and must be Service-Connected.
CATEGORY 2: Veterans who were assigned to a duty station in (including airspace above) certain locations during specific periods of time.
On or after August 2, 1990, in: Bahrain, Iraq, Kuwait, Oman, Qatar, Saudi Arabia, Somalia, or the United Arab Emirates
On or after September 11, 2001, in: Afghanistan, Djibouti, Egypt, Jordan, Lebanon, Syria, Yemen, Uzbekistan, or any other country determined relevant by VA.
CATEGORY 3: Veterans who deployed in support of Operation Enduring Freedom, Operation Freedom’s Sentinel, Operation Iraqi Freedom, Operation New Dawn, Operation Inherent Resolve, or Resolute Support Mission and other designated locations.
EFFECTIVE ON ENACTMENT (AUGUST 10, 2022):Veterans who served in the Republic of Vietnam (from 1/9/62–5/7/75), Thailand at any US or Royal Thai base (from 1/9/62–6/30/76), Laos (from 12/1/65–9/30/69), certain provinces in Cambodia (from 4/16/69–4/30/69), Guam, or American Samoa or their territorial waters (from 1/9/62–7/31/80), or the Johnston Atoll or a ship that called there (from 1/1/72–9/30/77) may enroll in VA health care.
BETWEEN OCTOBER 1, 2022, AND OCTOBER 1, 2023: Veterans who served on active duty in a theater of combat operations during a period of war after the Persian Gulf War or in combat against a hostile force during a period of hostilities after November 11, 1998, and who were discharged or released between September 11, 2001, and October 1, 2013, may enroll in VA health care. Enrollment is free, there are no annual costs, and healthcare may be free as well.
In addition a Veteran is eligible for a TERA Memorandum placed into their medical records if the participated in a TERA activity which includes:
Handling, maintain or detonating Nuclear Weapons
Working with radioactive material
Using calibration and measurement sources
Being exposed to X-rays
Being exposed to radiation from military occupational exposure
Being exposed to warfare agents
Being exposed to nerve agents
Being exposed to chemical and biological weapons
As of March 5, 2024, veterans who meet the basic service and discharge requirements and participated in a TERA are eligible to enroll in VA health care, FREE, without applying for VA benefits; meaning applying for some disability rating.
Contact your local Veteran Service Officer (VSO) offer for details. Be aware the benefit is through the Veterans Healthcare Administration (VHA) and is not the same as applying for disability with the Veterans Benefit Administration (VBA) a Disability rating entitling you to money. There is VA Form 10-10EZ to get and read the instructions. When this form is submitted along with any supporting documentation usually on the VBA-21-4138 it goes off to a separate address in Janesville, WI. Although you should think about applying for VA Disability Benefits ($$$) because you may well be entitled to it.
VA Added More Presumptive Conditions for Military Conflicts Since 1990
The VA has added Male Breast Cancer, Urethral Cancer and Cancer of the Paraurethral glands to the list of illnesses presumed connected to military service in conflicts since 1990. The policy change covers veterans who served in Southwest Asia. Veterans whose claims are approved may also be eligible for benefits back to August 2022 when the PACT Act of 2022 was signed. Survivors of those with these cancers maybe automatically granted financial payouts. (AirForce Times – July 2024)
More Disabilities Added to What the VA Will accept
This spring the VA announced an update to the VA Schedule for Rating Disabilities (VASRD) specifically pertaining to digestive conditions. The changes add or modify rating criteria for 55 medical conditions in the rating schedule that incorporate medical advancements for treating certain disabilities and modern medical knowledge to compensate Veterans more accurately.
The three biggest changes that will impact you, as Veterans, include the new evaluations for Celiac Disease, Irritable Bowel Syndrome (IBS) and Hemorrhoids.
Beginning May 19, Celiac Disease—an autoimmune disorder that impacts how the body processes gluten—will have its own rating criteria specifically designed to address its disabling effects. Veterans with this condition were previously granted service connection and evaluated by analogy using rating criteria that ranged from zero to 30 percent. Now under a specific diagnostic code, Veterans will be eligible for an evaluation ranging from zero to 80 percent.
VA will also adjust the rating criteria for evaluating Irritable Bowel Syndrome, also known as IBS. Previously, VA offered zero, 10 and 30 percent evaluations for the condition. Under the new criteria, Veterans may be entitled to 10, 20, or 30 percent evaluations based on the frequency of symptoms; therefore, new rating criteria will always offer a compensable evaluation.
Finally, VA addressed the evaluations for both internal and external Hemorrhoids. Previously, VA assigned a zero percent evaluation if the condition was identified as mild or moderate. For more severe findings a 10 or 20 percent evaluation was warranted. With the new rating criteria set in the rating schedule, mild or moderate hemorrhoids will now qualify for the 10 percent evaluation.
AnCan is grateful to the following sponsors for making this recording possible: Bayer, Foundation Medicine, Janssen, Myriad Genetics, Novartis, Telix & Blue Earth Diagnostics.
AnCan respectfully notes that it does not accept sponsored promotion. Any drugs, protocols or devices recommended in our discussions are based solely on anecdotal peer experience or clinical evidence.
AnCan cannot and does not provide medical advice. We encourage you to discuss anything you hear in our sessions with your own medical team.
AnCan reminds all Participants that Adverse Events experienced from prescribed drugs or protocols should be reported to the pharmaceutical manufacturer or the FDA Adverse Event Reporting System (FAERS). To do so call 1-800-332-1066 or download interactive FDA Form 3500 https://www.fda.gov/media/76299/download
AnCan’s Prostate Cancer Forum is back (https://ancan.org/forums). If you’d like to comment on anything you see in our Recordings or read in our Reminders, just sign up and go right ahead. You can also click on the Forum icon at the top right of the webpage.
All AnCan’s groups are free and drop-in … join us in person sometime!
Editor’s Pick: 1) Pluvicto pre-chemo… maybe? 2) Agree your stage before seeking treatment– rd
Topics Discussed
New denovo Nx Gent treated at VA gets less then SoC; get all docs to accept the same staging before seeking treatment; removing the surgical clip makes him feel better; 4x Pluvicto wasn’t enough – continues but is he concordant?; natural nausea remedies; intraductal/cribriform 4+5 Gent recurs 30 months post-RRP; extensive mets creep up on a Regular – Pluvicto pre-chemo?; gratitude!
JNJ-63898081 (JNJ-081) A bispecific antibody that targets PSMA on tumor cells and CD3 on T cells. JNJ-081 is designed to promote anti-tumor activity.
AnCan – rick
sent: 5:32 PM
Tx Len
Chuck Snyder
sent: 5:32 PM
Thanks all for the suggestions!
Len Sierra
sent: 5:41 PM
Aloxi (palonosetron) is another anti-nausea medication in the same class as ondansetron and granisetron (5HT3 antagonists).
Steve Roux, North Michigan
sent: 5:46 PM
hey guys, I need to run. Great Meeting, AGAIN. Don’t forget to get that survey done. Get ‘er done!
Chuck Snyder
sent: 5:46 PM
Thanks Len.
Len Sierra
sent: 5:50 PM
This is from AI, so understand the possible errors, but here is what they say: The choice of whether to use CTCs or ctDNA in a liquid biopsy depends on the specific clinical question being asked and the stage of cancer. For example, CTCs may be more useful for detecting early-stage cancer or monitoring the response to therapy, while ctDNA may be more sensitive for detecting advanced-stage cancer or identifying resistance mechanisms.
Julian – Houston
sent: 5:52 PM
• United States +1 (646) 749-3129
AnCan – rick
sent: 5:53 PM
222-583-973
Len Sierra
sent: 6:08 PM
I agree, great job, Dr. John!
Thomas M
sent: 6:09 PM
Was it Dr. Eshana Shah, MD at Fred Hutch who was mentioned?
Ancan would like your input on its future planning and academic research. Please take a few minutes to complete The 2024 AnCan Survey which is at thislink.
AnCan is grateful to the following sponsors for making this recording possible: Bayer, Foundation Medicine, Janssen, Myriad Genetics, Novartis, Telix & Blue Earth Diagnostics.
WELCOME all to our newly recorded Low/Intermediate Prostate Cancer Group. To receive notice when new recordings are posted, either follow us on this YouTube Channel or sign up to our Blog via https://ancan.org/contact-us/ – check New Blog box.
AnCan respectfully notes that it does not accept sponsored promotion. Any drugs, protocols or devices recommended in our discussions are based solely on anecdotal peer experience or clinical evidence.
AnCan cannot and does not provide medical advice. We encourage you to discuss anything you hear in our sessions with your own medical team.
AnCan reminds all Participants that Adverse Events experienced from prescribed drugs or protocols should be reported to the pharmaceutical manufacturer or the FDA Adverse Event Reporting System (FAERS). To do so call 1-800-332-1066 or download interactive FDA Form 3500 https://www.fda.gov/media/76299/download
AnCan’s Prostate Cancer Forum is back (https://ancan.org/forums). If you’d like to comment on anything you see in our Recordings or read in our Reminders, just sign up and go right ahead. You can also click on the Forum icon at the top right of the webpage.
All AnCan’s groups are free and drop-in … join us in person sometime!
Editor’s Pick: Prognostic tools are a good starting point for discussing treatment options with your doctors. (bj)
Topics Discussed
Online resources to compare multiple prognostic tools (e.g., nomograms, PSMA, NCCN) to diagnose our disease; initial considerations for treatment decisions, such as: some urologists view younger men as better candidates for surgery — be careful of this bias when considering your treatment options; PROSTOX saliva swab for germline DNA testing and avoiding toxicity from radiation therapy; getting the right information so you can make an informed decision; post SBRT urination problems include: frequency, urgency, and discomfort (burning, stinging, tingling); clarification on SBRT (a treatment) and Meridian (a radiation machine); urgency and incontinence; active surveillance; RTIRE trial acceptance; AnCan survey emailed to you — let us know what you think; a little humor with emotional support llamas; Happy Veterans Day.