Are you ready to get the inside scoop on clinical trials? Get ready to delve deep with former clinical trial nurse coordinator Marni Tierno. We know it can be a complex and overwhelming topic, but don’t worry – we’re here to break it down in a way that’s easy to understand.
Also featuring the vast professional experience of Wendy Garvin Mayo, we’ll tackle the myths and misconceptions that often surround clinical trials, giving you the facts and insights you need to make informed decisions.
Whether you’re a patient, carepartner, or simply curious about clinical trials, this webinar is for you! Our aim is to empower you with a deep understanding, allowing you to make the best choices for yourself or your loved ones.
Some of the topics we will cover include:
Description of the types and phases of clinical trials
Examples of pivotal clinical trials that have changed how we treat cancer
What to expect when participating in a clinical trial (including potential risks and benefits)
Addressing common questions about clinical trial participation
and more!
Watch here: (closed captioning is provided for this webinar, click the CC button at the bottom next to the gear.)
To view the slides from this webinar, please click here.
Special thanks to Bayer, Novartis, Johnson & Johnson, Foundation Medicine, Myriad Genetics, Telix, and Blue Earth Diagnostics for sponsoring this webinar.
And very special thanks to Illumina and Collaborative Cancer Care for letting us have two of their absolute best people present for us!
.
To SIGN UP for any of our Virtual Support groups, visit our Contact Us page.
Oh it’s not that kind of shot. It’s the other kind of shots, which require some modification for people with cancer. It just
so happens that ASCO (American Society of Clinical Oncology) has come out with new guidelines regarding vaccines for cancer patients.
The guidelines include a recommendation for doctors to take vaccination histories at the start of cancer treatment, followed by provision of recommended vaccines, re-vaccination after cancer treatments that wipe out immunity (for instance stem cell transplant), as well as vaccination of household contacts in order to protect the cancer patient.
We are more vulnerable to infection, because our immune system is injured by chronic inflammation, by the cancers, and by our treatments. Also, we don’t get as good an immune boost from some vaccines as people without cancer do.
If our immune system is “compromised” we can’t take live vaccines at all, and non-live vaccines aren’t as effective. Live vaccines contain weakened but still replicating virus or bacteria. They cause a mild infection in normal people, which triggers an immune
response. But for those of us with a weakened immune system, live vaccines, such as chicken pox/shingles, measles, mumps, oral typhoid, and German measles, can cause a real infection. Non-live vaccines are safe, including the new RNA vaccines. Non-live vaccines for different conditions can be given on the same day.
Here is a summary of recommendations, which I have shortened for prostate cancer:
“Clinicians should determine vaccination status and ensure that adults newly diagnosed with cancer and about to start treatment are up to date on seasonal vaccines as well as age- and risk-based vaccines
Vaccination should ideally precede any planned cancer treatment by 2-4 weeks. However, nonlive vaccines can be administered during or after chemotherapy or immunotherapy, hormonal treatment, radiation, or surgery
Adults with solid and hematologic cancers traveling to an area of risk should follow the CDC standard recommendations for the destination Note. Hepatitis A, intramuscular typhoid vaccine, inactivated polio, hepatitis B, rabies, meningococcal, and nonlive Japanese encephalitis vaccines are safe
It is recommended that all household members and close contacts, where feasible, be up to date on vaccinations “
Here are some specific recommended immunizations for adults with Cancer:
One dose of Tdap, followed by Td or Tdap booster every 10 years
Hepatitis B
19-59 years: eligible 60 years and older: immunize those with other risk factorsc
For adults 20 years and older, use high antigen (40 µg) and administer as a three-dose Recombivax HB series (0, 1, 6 months) or four-dose Engerix-B series (0, 1, 2, 6 months)18
Recombinant zoster vaccine
19 years and older
Two doses at least 4 weeks apart
Pneumococcal vaccine
19 years and older
One dose PCV15 followed by PPSV23 8 weeks later OR One dose PCV20d
HPV
27-45 years: shared decision making
Three doses, 0, 1–2, 6-monthsAbbreviations: HPV, human papillomavirus; PCV, pneumococcal conjugate vaccine; PPSV-23, 23 valent Pneumococcal polysaccharide vaccine; RSV, respiratory syncytial virus; Td, tetanus and diphtheria; Tdap, tetanus, diphtheria and pertussis.
a Live attenuated influenza vaccine, which is administered as a nasal spray, cannot be given to patients with cancer.
bTdap has lower amounts of diphtheria and pertussis toxoid and is only used for those 7 years and older. DTaP, the pediatric vaccine for prevention of tetanus, diphtheria, and pertussis, is only for children younger than 7 years.
cHIV, chronic liver diseases, intravenous drug use, sexual risk factors, incarcerated individuals.
dPatients who have previously received PCV13 only can receive one dose of PCV 20 after an interval of 1 year.
Abbreviations: HPV, human papillomavirus; PCV, pneumococcal conjugate vaccine; PPSV-23, 23 valent Pneumococcal polysaccharide vaccine; RSV, respiratory syncytial virus; Td, tetanus and diphtheria; Tdap, tetanus, diphtheria and pertussis.
a Live attenuated influenza vaccine, which is administered as a nasal spray, cannot be given to patients with cancer.
bTdap has lower amounts of diphtheria and pertussis toxoid and is only used for those 7 years and older. DTaP, the pediatric vaccine for prevention of tetanus, diphtheria, and pertussis, is only for children younger than 7 years.
cHIV, chronic liver diseases, intravenous drug use, sexual risk factors, incarcerated individuals.
dPatients who have previously received PCV13 only can receive one dose of PCV 20 after an interval of 1 year.
Now, a few further details about some common shots:
COVID
The COVID-19 vaccines protect patients with cancer, reducing the risk of severe COVID-19 illness and hospitalization. The recommendation is to receive at least one dose of the updated 2023-2024 COVID-19 vaccine. For those on therapies which diminish the immune response, ASCO recommends additional vaccine doses after 2 months. It is recommended to postpone immunization for 2-3 months for individuals who have recently had a COVID-19 infection.
FLU
It is safe to vaccinate during chemotherapy or while white cells are low. But the nasal spray flu vaccine should not be given to patients with cancer.
Pneumonia
Patients with cancer are at higher risk for pneumonia. (Blood cancers 50 times the risk!) Pneumonia vaccines reduce the chances of getting pneumonia and the need for hospitalization.
Shingles
There is a new vaccine called RZV. It is non-live so OK for us. (the previous vaccine, a live attenuated type, is not recommended for patients with cancer.) RZV should be made available to all adults with cancer. This vaccine remains immunogenic even after cancer treatment has begun.
RSV
Patients aged 60 years and older with cancer are eligible to receive the respiratory syncytial virus vaccine.
Our immunity to tetanus, diphtheria, and pertussis weakens as we age, and this decline may be accelerated after cancer treatment. It is strongly recommended that individuals diagnosed with cancer receive the Tdap vaccine if they have not been vaccinated as adults.
Why bother?
“Infections are the second most common cause of non–cancer-related mortality within the first year after a cancer diagnosis, with most of these deaths attributed to influenza and pneumonia, deaths that can be prevented throughimmunization. While patients with cancer have lower immune responses to influenza and pneumococcal vaccines, evidence supports the safety and benefits of vaccinations in reducing the severity of infections and associated hospitalizations.”
Often we will see the term “immunocompromised.” Does this apply to us? This term is not, to my knowledge, precisely defined. For those of us with prostate cancer, it usually means neutrophils (a type of white blood cell) are down below 1000 cells per microliter of blood, and is usually due to our treatments. The immune system is complex, and there are many ways to become “immunocompromised.” Anyone on chemotherapy could be considered to be immunocompromised. .Ask your oncologist if you fit this category, and if you know of a clear generally accepted definition, please write to me.
The authors sum up: “A cancer diagnosis can be overwhelming, and vaccination may not be an immediate priority in the treatment plan. However, numerous studies consistently highlight the best protection when vaccines are administered before starting cancer treatment, emphasizing the need for early vaccination.”
AnCan Foundation supports several conditions that compromise the pelvic floor as a result of surgery, radiation, or just side effects of the disease itself. It can impact continence and sexual function for all!
A non-interventional rehab solution is pelvic floor physical therapy – a sub-specialty in itself.
Join one of AnCan’s favorite superstars, urologist Dr. Rachel Rubin, and esteemed expert Dr. Tracy Sher. Together, shared how pelvic floor exercises can help you recover function!
You’ll also get a ton of questions answered, asked by MS Moderator Kim Stroeh, and Prostate Cancer moderator Dr. John Antonucci.
Watch here:
Special thanks to Bayer, Pfizer, Myovant Sciences, Foundation Medicine, Myriad Genetics, Janssen – Johnson & Johnson, and Telix for sponsoring this webinar.
Check back later for slides.
For information on our peer-led video chat VIRTUAL SUPPORT GROUPS, click here.
To SIGN UP for any of our Virtual Support groups, visit our Contact Us page.
(Editor’s note: This is a ‘master’ list of books related to death, dying, and grief. We hope you will find this to be a helpful resource in your journey, no matter what it is. If you would like to share a book that has helped you, please email alexa at rickd13.sg-host.com. Amazon links here for your convenience and ease of purchasing the book. Remember, you can help AnCan with absolutely no cost to you by purchasing through AmazonSmile. Read how to here. Special thanks to Dr. John Antonucci.)
“We face fears of death and dying, and at times turn to authors who have thought deeply and written about the topic. I offer here a short bibliography on the topic. Ideally it would be an organic list, onto which readers could add suggestions or comments.” – Dr. John Antonucci
Today’s a BIG DAY if you’re a fan of ordering everything you need from Amazon.
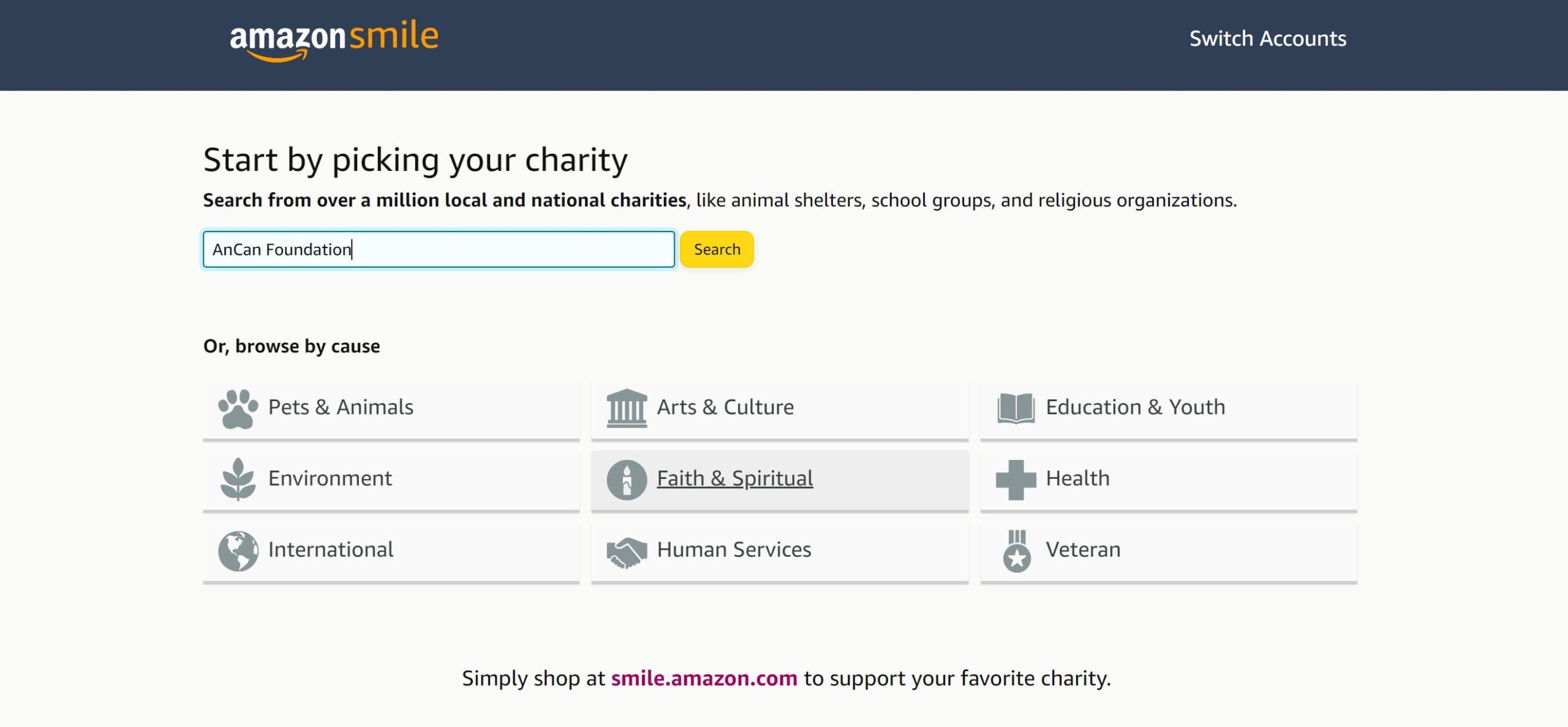
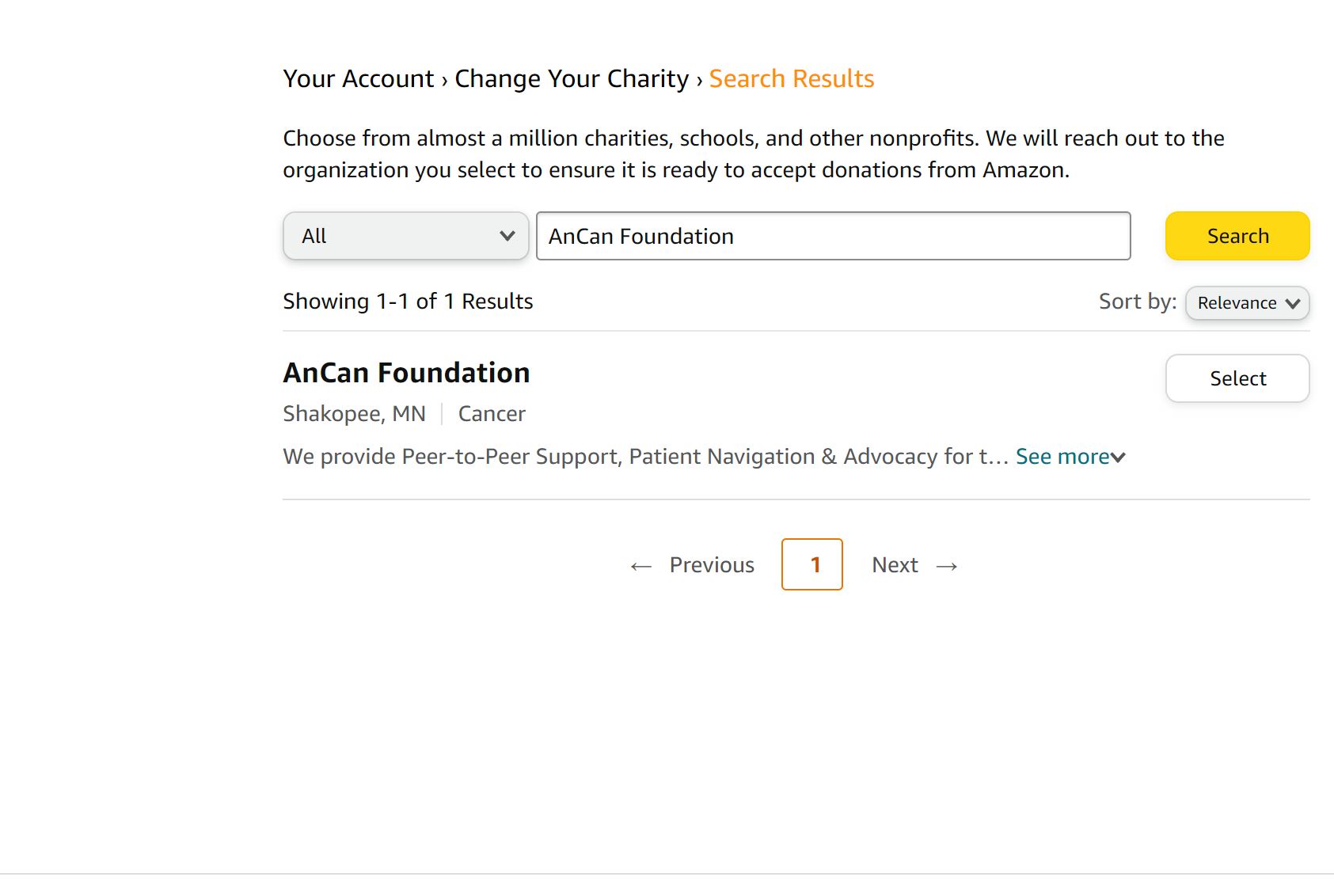
October 11-12th are Amazon Prime Early Access Days, and guess what? If you sign up for Amazon Smile, you can give back to us without having to spend anything extra! It sounds too good to be true, but it absolutely is real.
Amazon will donate .5% of eligible purchases to the organization YOU choose. That could be us…we would be grateful for it, and you would be helping us provide quality peer-to-peer support for all AnCan-ers.
In case you’re new or need a reminder:
We’re a peer-to-peer organization that provides support to many different conditions – Prostate Cancer, Multiple Sclerosis, Sarcoidosis, Thyroid Cancer – quite literally just to name a few. We also host many a webinar – all in the name of support for our community and groups. Check out our YouTube page for past recordings.





 Oh it’s not that kind of shot. It’s the other kind of shots, which require some modification for people with cancer. It just
Oh it’s not that kind of shot. It’s the other kind of shots, which require some modification for people with cancer. It just