by Kiernan Mehan | Feb 23, 2026 | Active Surveillance PCa, Advocacy, Cancer Caregivers, Cancer Resources, Exercise, Low/Intermediate Prostate Cancer, mCRPC, Men 'Speaking Freely', Mental Health, mHSPC, Nutrition, Press, Prostate Cancer, Recent News, Uncategorized

AnCan GU ASCO26 survivorship poster: participants strongly endorse our Groups
For release on Monday, Feb 23, 2026
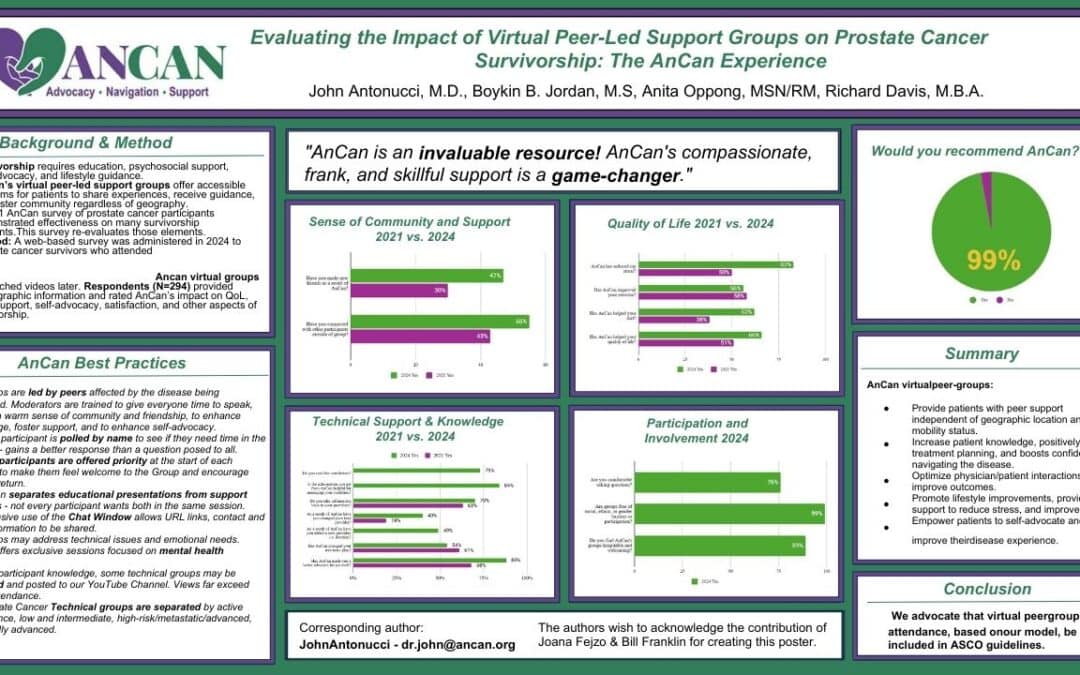
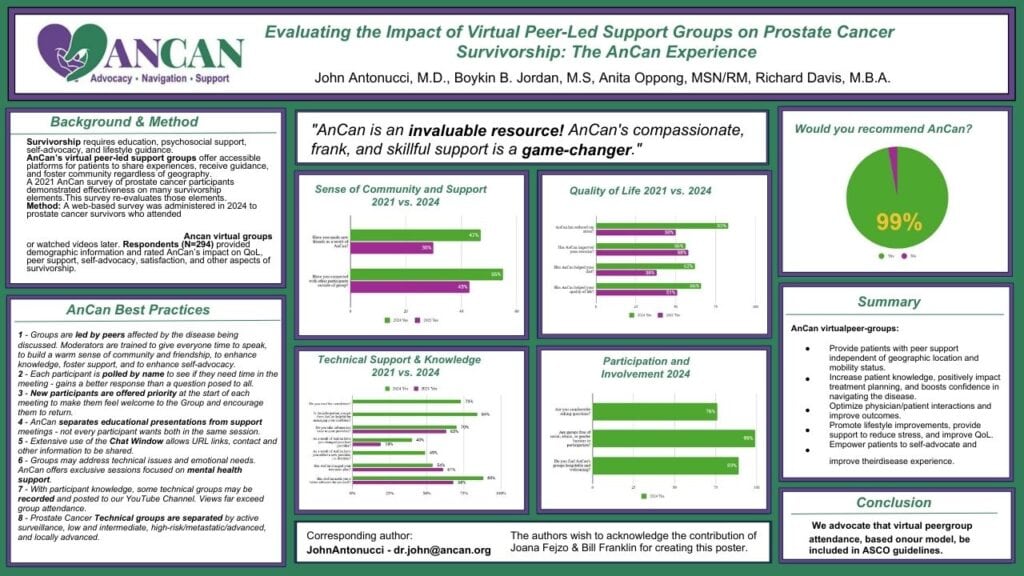
AnCan Foundation strongly believes we run the best support groups available!! We can now release the first results of our 2024 AnCan Participant Survey that confirms that our participants think so too. This first batch of results is taken from almost 300 prostate cancer responses at all levels of disease.
- 99% of respondents would recommend AnCan Groups
- 66% improved Quality of Life – 83% noted reduced stress; 62% improved nutrition; 56% increased exercise
- 88% advocated better for themselves and AnCan influenced over half (54%) the treatment paths
- 47% made new friendships – AnCan’s personal favorite since this extends support well beyond our Groups
If you’re attending GU ASCO26 , please stop by our poster on Friday, Feb 27 to meet Dr. John Antonucci, discuss these astonishing results and the AnCan method, and pick up a flyer of the poster.
CONTACT


ABSTRACT
Evaluating the impact of virtual peer-led support groups on prostate cancer survivorship: the AnCan experience.
John Antonucci*, Boykin B. Jordan, Anita Oppong, Richard Davis
- Abstract Number: 265
- Poster Board Number: A23
- Session Title: Poster Session B: Prostate Cancer and Urothelial Carcinoma
- Date and Time: February 27, 2026, 11:30 AM-12:45 PM; 4:45 PM-5:45 PM (PST)
Background: Comprehensive prostate cancer (PCa) survivorship requires more than just clinical care, including education, psychosocial support, self-advocacy, and lifestyle guidance—needs often unmet by traditional oncology visits. Virtual peer-led support groups, such as those offered by the AnCan Foundation, offer accessible, real-time platforms for patients to share experiences, receive guidance, and foster community, regardless of geography. This study evaluates the impact of AnCan participation on factors known to be associated with a better quality of life (QOL) among PCa survivors.
Methods: A web-based survey was administered in 2024 to PCa survivors who attended or expressed interest in AnCan meetings. Respondents (N=294) provided demographic information and rated AnCan’s impact on QOL, peer support, self-advocacy, and satisfaction. Data were analyzed to assess the subjective influence of AnCan’s virtual support model on survivorship.
Results: (2021 results are in brackets for comparison.) Most respondents were in their 60s–70s (75%), highly educated (82%), and 55% had incomes over $100,000. Eighty-three percent had someone in their lives they could rely on and with whom they maintained regular contact.
Nearly all (97%) found AnCan meetings helpful for disease understanding, learning options, and well-being. Sixty-six percent reported improved QOL; 83% [50%] noted reduced stress; 62% [38%] improved nutrition; and 56% [58%] increased exercise. Satisfaction was high, with 99% recommending AnCan.
AnCan involvement enhanced self-advocacy (88%), improved patient-provider communication, and improved decision-making. Seventy percent brought information from AnCan to their providers, 49% added new providers, and 40% changed their lead provider. Over half (54%) reported that AnCan influenced their treatment path.
Socially, 55% [43%] connected with peers outside meetings, and 47% made new friendships.
Conclusions: Survey responses indicate that the AnCan virtual peer-led model, to be described in the poster, meaningfully increases patient knowledge, empowers self-advocacy, reduces stress, and fosters healthy behaviors, improving quality of life for PCa survivors. We advocate for integrating such peer support into NCCN, AUA, and ASCO survivorship guidelines.
POSTER
by Kiernan Mehan | Dec 28, 2025 | Advocacy, Cancer Resources, Press, Recent News
Empowered Patient Podcast: Virtual Support Groups Remove Barriers Encourage Sharing Honest Experiences to Fight Misinformation with Rick Davis, AnCan
AnCan founder, Rick Davis, was recently featured in the Empowered Patient Podcast with Karen Jagoda. This show explores the cutting edge of healthcare, highlighting innovations in generative AI and the latest breakthroughs in therapeutics and vaccines, and explores a shifting landscape where providers, pharma, and payers are prioritizing patient empowerment.
Rick explains, “The mission is to make each person and each patient a better advocate for themselves. That’s really what we try to do, and we do that through empowering patients with peer knowledge. We introduce patients to other peers who have been through what these people are facing right now, not only patients, but also their care partners, and through their experience, we hope that these patients and care partners will become more expert in managing their own situation.”
If you have 20 minutes, click here to listen to the podcast. If you’d like to read the conversation, click here for the transcript.

by Alexa Jett | Jun 17, 2025 | Press, Prostate Cancer, Recent News, RMC, Volunteers
AnCan, is proud to announce that two of its dedicated patient advocates have been named to the esteemed Cancer Health 25 list. This annual recognition by Cancer Health magazine salutes outstanding individuals who are making a profound difference in the lives of those affected by cancer.
The Cancer Health 25 list highlights the unwavering efforts of patient advocates who bridge critical gaps in cancer care, providing essential support, education, and resources. As the article states, “No one should face cancer alone. Luckily, a vast range of skilled and dedicated patient advocates can provide support to people with cancer and their loved ones.” The list acknowledges individuals who raise funds and awareness, build programs, share information, facilitate access to care, and much more, especially for vulnerable and underserved communities.
We are incredibly honored to see two of our own advocates recognized among such an inspiring group of individuals. This recognition underscores the vital role that patient advocates play in ensuring that no one walks their cancer journey alone. Our advocates tirelessly embody Dr. Harold P. Freeman’s vision of filling the ‘disconnect between what we discover and what we deliver’ in cancer care. We are immensely proud of their dedication and the profound impact they have every day.

Ritchie Johnson
Among those recognized is Ritchie Johnson, MBA, RN, founder of the Chris “CJ” Johnson Foundation and co-founder of AnCan’s Renal Medullary Carcinoma (RMC) virtual support group. Ritchie launched the Chris “CJ” Johnson Foundation in memory of her son, who died of RMC, a rare and aggressive type of kidney cancer primarily affecting young African Americans with sickle cell trait. A relentless advocate, Johnson has tirelessly pushed for increased RMC awareness, funding, and scientific attention, which has led to the formation of multiple clinical trials.
Howard Wolinsky
Also honored is Howard Wolinsky, a Pulitzer Prize–nominated medical journalist and a prominent advocate for active surveillance in prostate cancer. Diagnosed with low-risk prostate cancer at 63, he chose active surveillance over immediate treatment 15 years ago and has not yet required intervention. He passionately supports others navigating similar decisions, co-authoring dozens of articles in medical journals with physician-scientists. He is the editor of TheActiveSurveillor.com and is a co-founder of our Active Surveillance Prostate Cancer Group.
Our mission is rooted in the belief that shared experiences and peer support are fundamental to navigating a cancer diagnosis. The organization’s advocates work diligently to connect patients and caregivers, provide trusted information, and foster a strong, supportive community. Their inclusion in the Cancer Health 25 is a testament to their commitment and the effectiveness of AnCan’s patient-centric approach.
AnCan extends its deepest gratitude to Cancer Health for shining a light on the invaluable contributions of patient advocates and for recognizing the tireless efforts of its team members.
by Rick Davis | May 16, 2022 | Active Surveillance PCa, mCRPC, nmCRPC, Press, Prostate Cancer, Recent News
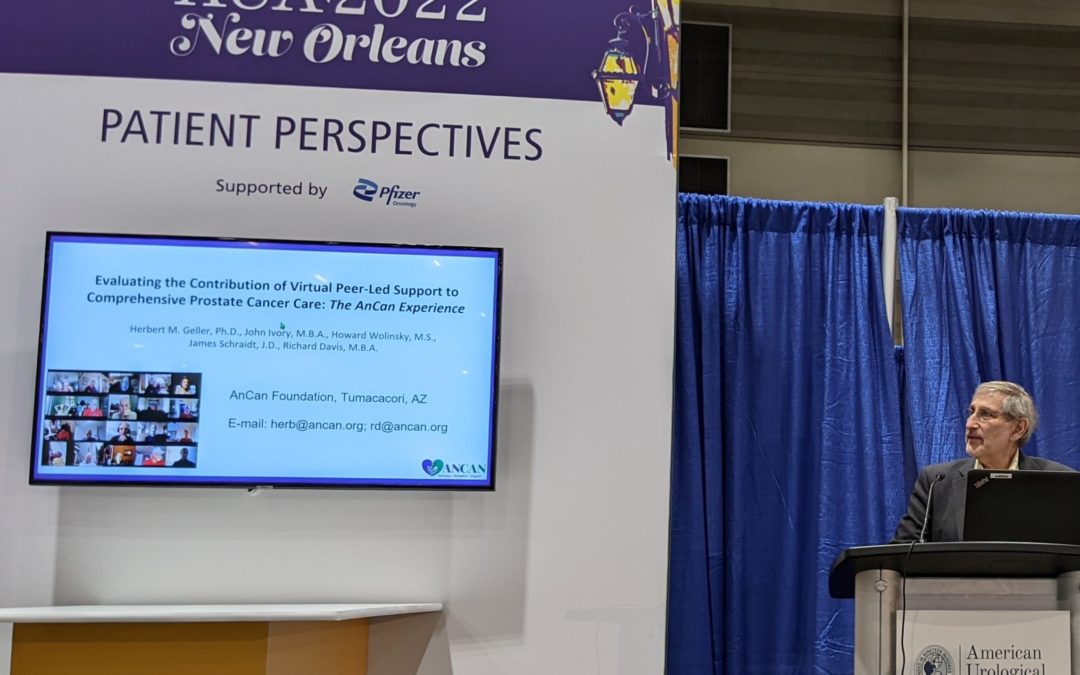
AnCan Goes Live! … at AUA22 in N’awlins

Herb in AnCan’s Glory
Live performances: Many of us have missed them for two long COVID years. New Orleans has especially missed them. And while AnCan may have never missed them, given our virtual model, Herb Geller still rocked a standing-room-only, live crowd at the American Urological Association (AUA) Annual Conference last Friday the 13th (a good omen, in this case).
Herb delivered AnCan’s research, “Evaluating the Contribution of Video Peer-Led Support to Prostate Cancer Patients: The AnCan Experience” as part of the AUAs “Patient Perspectives” program.

John Ivory, Herb Geller & Jim Schraidt
A number of you with prostate cancer will remember helping us by taking one or two online surveys last year, which made this research possible. Parts of this research had already been accepted at two other conferences, the European Society for Medical Oncology (ESMO) and American Society of Clinical Oncology (ASCO). While we were pleased to be recognized by those forums, COVID turned those conferences virtual, and there’s nothing like a live performance. Herb presented our greatest hits combining both the overall survey and our Active Surveilance specific questionnaire.
Survey participants said this about AnCan groups:
- 83% agreed the information is useful
- 67% discussed the information with their care teams
- 61% changed or informed their treatment path or strategy
- 71% found help navigating treatment path or strategy
- 80% became better advocates for themselves
Strikingly, AnCan participants have improved their lifestyle habits:
- 58% improved exercise habits
- 38% improved diets
- 50% reported reduced stress
AnCan helped participants make connections with each other:
- 85% found the groups to be welcoming
- 43% connected with others
- 30% developed friendships with other participants
Among those who attend early diagnosis, low-risk Active Surveillance meetings:
- 68% said that attendance helped them be their own best advocate
- 23% said that attendance informed them of new insights and treatments
AnCan concluded that:
- The AnCan Support Group model increases patient knowledge, positively impacts treatment planning, and promotes lifestyle improvements while providing support to reduce stress, boosts confidence in navigating the disease, and improves quality of life.
- AnCan empowers patients to self-advocate and improve their disease experience. This is integral to optimize physician/patient interactions and improve outcomes.
- We advocate that virtual peer group attendance, based on our model, be included in (National Comprehensive Cancer Network) NCCN treatment recommendations for prostate cancer patients, especially with advanced disease.
If you took part in one of the two surveys, thanks again. And thanks especially to Rick Davis, Herbert M. Geller, James Schraidt, Howard Wolinsky, (and yours truly) for designing the surveys, crunching the data, and developing and presenting the insights from the data.
John Ivory, May 15 2022

by Alexa Jett | Feb 17, 2022 | Advocacy, Press, Recent News
AnCan Recognized by GU ASCO22 For Peer Led Support Groups
AnCan Foundation is honored to announce its Abstract #58: Evaluating The Contribution of Virtual Peer-Led Support to Comprehensive Prostate Cancer (PCa) Care: The AnCan Experience together with a virtual poster has been selected for the ASCO Genitourinary Cancers Symposium, Feb 17-19, 2022 in San Francisco. DOI: 10.1200/JCO.2022.40.6_suppl.058
AnCan’s founder, Rick Davis, innovated virtual peer-led support groups back in 2010. He recognized the potential of peer advice as the best information a patient could find. AnCan’s 2021 research confirms what Rick knew intuitively.
Neuroscientist Herb Geller PhD, the abstract’s lead author, highlighted the following key research findings,
“Our research indicates that peer-led groups don’t just improve quality of life around the things we can control like diet, exercise and stress. Eighty percent of our participants feel the groups make them better advocates for themselves, and well over 60% take information gleaned back to their healthcare teams.”
While this poster is featured in the Advanced Prostate Cancer track on Feb 17, AnCan is proud of its work to establish the stature of the low risk Active Surveillance (AS) protocol and includes its AS findings.
Co-author and nationally recognized AS Advocate, Howard Wolinsky, said:
“Sixty eight percent of our AS participants told us the Groups made them better advocates and 27% reported lower levels of anxiety – that’s a major difference. Active surveillance is the Rodney Dangerfield of prostate cancer – including our study at GU ASCO recognizes AS patients”
Rick Davis, founder of AnCan and a prostate cancer survivor, says the research demonstrates the power of patient communities on outcomes:
“I realized the power of peer-led support groups from my own treatment. Bringing them to a virtual platform 10 years before anyone had ever heard of COVID-19 and Zoom meetings, made peer support available to those compromised by geographical, physical and social issues. Recognition by GU ASCO is a big step in legitimizing AnCan’s work for all peer-led support.”
View full press release here,
View the poster here.
For information on our peer-led video chat VIRTUAL SUPPORT GROUPS, click here.
To SIGN UP for any of our groups, visit our Contact Us page.

by Rick Davis | Oct 23, 2020 | Webinars, mCRPC, nmCRPC, Press, Prostate Cancer, Recent News
AnCan & Patient Power partner for Prostate Cancer Webinar Series


Answering your Prostate Cancer Questions
To watch these seminars, folow these links:
“Prostate Cancer and Making Sense of nmCRPC Options” – Rick & Len speak with Drs. Eleni Efstathiou and Tom Beer
“PSA Test & Imaging for Prostate Cancer Patients” – Len & Peter Speak with Drs. Scott Tagawa and David VanderWeele
“How to Manage Side Effects & Reduce Suffering” – Peter and Rick speak with Dr. Atush Choudhury –
Three of AnCan’s senior and most knowlegeable prostate cancer moderators, Len Sierra, Peter Kafka and Rick Davis, team up to host and interview five expert and renown genitourinary medical oncologists in three separate webinars during October and November. Len, Peter & Rick along with Jake Hannam moderate AnCan’s 4 times per month High Risk/Recurrent/Advanced Prostate Cancer video chat virtual support group.
Our hosts will be interviewing:
Eleni Efstathiou MD, PhD
Associate Professor, Department of Genitourinary
Medical Oncology, Division of Cancer Medicine,
The University of Texas MD Anderson Cancer Center
Tomasz Beer MD, FACP
Deputy Director, OHSU Knight Cancer Institute
Scott T. Tagawa MD, MS, FACP
Professor of Medicine and Urology, Weill Cornell
Medicine; Physician, NewYork-Presbyterian -Weill Cornell Medical Center
David VanderWeele MD, PhD
Assistant Professor of Medicine, Northwestern
University Feinberg School of Medicine; Medical
Oncologist, Lurie Cancer Center at Northwestern Memorial Hospital
Atish D. Choudhury MD, PhD
Co-Director of the Prostate Cancer Center,
Dana-Farber Cancer Center
For dates, topics and live registration links to each webinar, click Patient Power AnCan CRPC Series
