
by Rick Davis | Feb 19, 2026 | Active Surveillance PCa, Advocacy, Blood Cancers, Cancer Caregivers, Cancer Resources, Health Resources, Men's Breast Cancer, Pancreatic Cancer, Prostate Cancer, Recent News, Thyroid Cancer, Uncategorized
Telehealth gets extended through 2027!
As some of you may know, the liberal telehealth rules to conduct medical appointments remotely that were enabled during Covid, sunsetted late last year. AnCan was upset and vocal that many of our patient advocacy organizations active on The Hill did not campaign more widely to extend it. Organizations like ZERO (prostate cancer) have significant and expensive government relations groups precisely to address such issues on behalf of us patients. AnCan had to bring it to ZERO’s attention to move the ball at a time when ZERO’s high paid CEO was self-admittedly sleeping on the switch.
Telehealth was temporarily extended for those living in rural areas. Then one of our newly minted prostate cancer Moderators, David Sharpe, brought it to AnCan’s attention that legislation was passed on Feb 3, 2026 that has extended comprehensive telehealth through the end of 2027. We asked David to blog its welcome return to wider availability and tell his story around telehealth – thank you Mr. Sharpe!
Medicare Telehealth Coverage Is Extended
The federal government has restored Medicare coverage for telehealth until the end of 2027. That means you can now possibly consult with your doctors online rather than having to meet with them in-person.
Why did I say possibly? Because state medical licensing laws still apply. Often, they can undermine your doctor’s ability to join you on the call. Here’s why: (Don’t construe the following comments as legal or medical advice. This is general information only.)
Telehealth consultations are easiest to arrange when a patient and doctor are in the same state. For instance, if you live in Springfield, Illinois, and want to have a virtual chat with an oncologist in Chicago, no legal impediments are likely to stand in your way.
Things can get tougher if the doctor practices in another state. Physicians are typically required to be licensed in the state where the patient is physically located during the consult. Therein lies a common problem: the doctor is licensed in one state, and you’re in another.
But loopholes exist. According to the Center for Connected Health Policy (CCHP), “A few states have licenses or telehealth-specific exceptions that allow an out-of-state provider to render services via telemedicine in a state where they are not located, or allow a clinician to provide services via telehealth in a state if certain conditions are met (such as agreeing that they will not open an office in that state). Still other states have laws that don’t specifically address telehealth and/or telemedicine licensing, but make allowances for practicing in contiguous states. . . .” For specifics about your state’s rules, explore CCHP’s handy state-by-state guide: https://www.cchpca.org/topic/cross-state-licensing-professional-requirements/.
Despite those exceptions, many physicians and medical centers require patients to be in the same state as the doctor during telehealth appointments. I wish I’d known that last year, before trying to set up virtual consultations from my home in Portland, Oregon, with Fred Hutch (Washington), UCSF, City of Hope (both California), and MD Anderson (Texas0—all of whom turned me down. Oregon Health & Science University (OHSU, Oregon)) would have refused, too, if I had been in any other state.
But some physicians and hospitals were more relaxed about it. Despite remaining in Portland, I wrangled a telehealth visit with a UCLA specialist. Two AnCan buddies of mine in Oregon and Arizona did so as well. I had even better luck with out-of-state doctors in community practices. Two agreed to confer with me online, and one declined.
If you live near—but not in—the state where your doctor practices, perhaps the easiest option is to make a run for the border. One AnCan member has adopted that strategy as a convenient means of communicating with his faraway medical team in an adjacent state while also satisfying the legal requirements. To have that meeting, he travels a few miles from home to a casino just across the state line; the casino lets him conduct telehealth consultations there. That approach shaves hours off what would otherwise be a protracted road trip to talk with his doctors face-to-face. # # #
David Sharp davidsharp1@me.com
by Alexa Jett | Nov 24, 2025
This group provides a chance for individuals under 45 (or around that age) with MS to share common experiences and concerns, provide and receive emotional support, and get information on various aspects of living well with MS. We often feel that the things we face when we’re younger can be different. Meetings are open to anyone, regardless of location.
4th Thursdays of the month – 7:30 pm
by Rick Davis | Oct 28, 2024 | Active Surveillance PCa, Blood Cancers, Cancer Caregivers, Cancer Resources, High Risk/Recurrent/Advanced, High Risk/Recurrent/Advanced Prostate Cancer, Low/Intermediate Prostate Cancer, mCRPC, Men's Breast Cancer, Multiple Sclerosis, nmCRPC, Ovarian Cancer, Pancreatic Cancer, Prostate Cancer, Recent News, RMC, Thyroid Cancer, Uncategorized
More on Medicare 2025: Drug Costs
UPDATE – PLEASE SEE IN PURPLE AT THE BOTTOM
A couple of weeks back, we posted Medicare Health Insurance Choices that explained the differences and pitfalls between traditional Medicare Part A and B plus Medigap insurance plans to Part C, Medicare Advantage. Click the link earlier in the previous sentence if you missed it.
As many already know, there is a Part D that covers drug costs. It is either purchased as a separate plan or rolled into Part C Advantage. Drug coverage is significantly changing this year, and AnCan has learnt that many of our participants are not yet aware. Hardly surprising because CMS as well as the various stakeholders like Payers and providers have done very little to let us patients know. Why should they? – we’re only the ultimate consumer!
The same cannot be said of JnJ who started educating patient advocate organizations this past May. In October and November JnJ created more education that includes a webinar and a round table coming up hosted by NAMAPA, the National Association for Medication Access and Patient Advocacy. Likely you have never heard of them. I hadn’t and it hardly rolls off the tongue. Nonetheless, the webinar was very instructive and you can watch it here.
The BIG difference for us patients is that no matter what, out-of-pocket drug costs for 2025 cannot exceed $2000. You heard right – for those of you on specialty oral medications like Nubeqa (darolutamide for prostate cancer) or Aubagio (teriflunomide for MS), normally sourced via specialty pharmacies, you will meet this cap January. And you’ll even be able to spread the payment over 12 months! More on that to follow.
But first, how is this coming about. Well it tracks back tot he changes brought about by the Inflation Reduction Act signed by President Biden in 2022. He promised to make drugs more affordable, 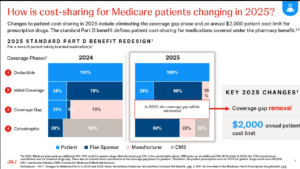 and this is a part of the plan. As you can see in the slide to the left comparing 2024 to 2025, the donut hole has been eliminated. In its place, the Payer (Plan Sponsor) and Pharma (manufacturer) are paying more. While the cost saving is very positive, it will likely impact us patients in other ways:
and this is a part of the plan. As you can see in the slide to the left comparing 2024 to 2025, the donut hole has been eliminated. In its place, the Payer (Plan Sponsor) and Pharma (manufacturer) are paying more. While the cost saving is very positive, it will likely impact us patients in other ways:
- Your formulary choice may be reduced – so CHECK your medications before you renew.
- Premiums for Part D may increase – even though out of pocket is capped. If you are unlikely to spend $2,000, look for a plan that defers your co-pay as long as possible
- Higher premium plans should cover a larger portion of drug costs earlier. Your premium does NOT count towards the $2,000, so include premiums in your cost calculation to figure your exposure.
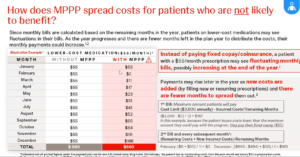
If you have a co-pay or co-insurance on your drugs, no matter if it’s Part C or D, it cannot exceed $2,000. However the amount you pay and who you pay it to may become a bit of a moving target. We mentioned earlier that you will now have the opportunity to spread your payments over the calendar year – or the remainder of it, if you sign up late or incur costs late in the year. The Medicare Prescription Payment Plan (M3P) takes your share of drug costs, up to a maximum of $2,000, and spreads them over the remainder of the year.
The simple example is for those on specialty pharmaceutical drugs like Nubeqa or Aubagio. Since your share of the drug cost is almost certainly going to be greater than $2,000 in January, if you opt in for M3P BEFORE going to the pharmacy or ordering from your mail order pharmacy, you’ll pay nothing on picking up/shipping the drugs. Subsequently, you’ll get a separate bill from your Payer for $167.67 monthly over 12 months, and pay no more for any of your drugs the rest of the year. There is NO interest, no late fee penalties, and you get a couple of months leeway, but there are penalties if you never pay. You can sign up for MP3 with your Medicare Payer/Plan Holder BUT not in the pharmacy for 2025. So if you arrive at the drug store prior to enrollment, you’ll be charged $2,000 to take your pills home. You can leave the pills, go home, enroll and return to the pharmacy 24 hours later and pick up without payment to the pharmacy..
If you don’t start this expensive drug until mid year, say September, and you’ve spent nothing on drugs prior, then the $2,000 is billed over the last 4 months at $500/month.
 But what if your drug costs are more lumpy – they go up and down the whole year. In that case, the payments get recalculated each month and the monthly bill will vary.
But what if your drug costs are more lumpy – they go up and down the whole year. In that case, the payments get recalculated each month and the monthly bill will vary.
There is a strange case too, if you know your co-pay is the same each month – say $55. This really throws M3P, and as you can see to the left, you’ll pay the same $660 (12x $55) either way but in different amounts each month if enrolled in M3P.
Finally, let’s address the Drug Benefit plans that many of you enjoy through PAN, PAF and others. Even the drug discount cards from Pharma that some receive. Whatever you receive, or however you receive it, does NOT reduce your $2,000 exposure. You advise the pharmacy that you have a benefit, and they bill the Benefit Provider (PAN, PAF, Pharma ??). The credit will be applied against your drug cost, although eventually you may still be liable for up to $2,000 co-pay when the benefit runs out.
Looking at the first slide, it seems to AnCan that these benefits that are often funded by Pharma, eventually flow back to Pharma and the Payer. How they will credit them against what the patient owes is not yet clear. Before you get too crazed, our guess is the system has to change. These benefits need to be channeled directly to patients who cannot afford $2,000 p.a. AnCan is on it and already reaching out to NAMAPA and others to promote more of a direct, income based subsidy possibly reaching more beneficiaries. One thing we have heard – APPLY EARLY for 2025 in the event you are in line to receive a subsidy.
Attribution: UPDATE – Slides are now available at Understanding Medicare Part D Changes and Their Impact on Patient Out-Of-Pocket Costs in 2025 prepared by JnJ and presented by NAMAPA and JnJ.!!
PLEASE BE SURE TO SIGN UP FOR THE M3P PROGRAM UPFRONT. EVEN IF YOU OWE $2,000 IT WILL BE BILLED IN 12 INSTALLMENTS. WE STILLL HAVE TO FIGURE HOW YOU WILL BE REIMBURSED IF YOU RECEIVE ASSISTANCE.
IF YOU HAVE A GRANT BE SURE TO PROVIDE DETALS TO THE PHARMACY ASAP. NOTWITHSTANDING, ALSO REACH OUT TO YOUR GRANTOR TO FIND HOW THEY WANT TO COORDINATE THE GRANT. IT’S STILLL A MOVING TARGET!
by Rick Davis | Jul 29, 2024 | Active Surveillance PCa, AYA, Blood Cancers, Brain Tumors, Cancer Caregivers, Cancer Resources, Complementary Medicine, Health Resources, Low/Intermediate Prostate Cancer, Men's Breast Cancer, Multiple Sclerosis, Ovarian Cancer, Pancreatic Cancer, Prostate Cancer, Recent News, RMC, Sarcoidosis, Thyroid Cancer, Women's Breast Cancer
Helpful Tips to be Your Own Best Medical Researcher
AnCan asked Mike Wyn, a valued AnCan Frequent Flyer and intrepid researcher, to provide a little navigation to those who are new to research… as well as useful tips for some old hands like myself. I’ve already gathered some research nuggets from Mike’s wisdom… thank you, Mr. W.
Here are a few tips ensure the medical information you are researching is reliable and accurate
Book Research
Check the publication date: authors may need at least a year to write a book, and the average time between a book’s acceptance and its publication is typically between 9 to 12 months. Hence, the data may already be outdated when it hits the shelves
Professional Presentations
Check the credentials, disclaimers, and disclosures of the presenters. Who is the author? What is the sponsoring organization providing the information? Preferred sources are from reputable institutions, such as universities, hospitals, or government health agencies.
Google Web Searches
Use command “site:” to limit you search to top-level domains like .gov, ,org and ,edu. For example, type: latest NCCN guidelines for prostate active surveillance site: .gov OR site: .org OR site: .edu
Be cautious with .com sites unless they are from recognized and credible entities. Medical databases such as PubMed, Cochrane Library, and Google Scholar are good sources for cross-referencing scientific research.
Articles, Online Posts
Check articles, online posts, videos etc. for their sources, including scientific studies, medical journals, or clinical trials. Information from peer-reviewed journals is typically more reliable than content from non-peer-reviewed sources. Poor reviewed means that other people similarly qualified to the author have reviewed teh article adn provided comments.
Anecdotal Evidence
Anecdotal evidence is information that has been observed by the person reporting but not verified. Be skeptical of anecdotal evidence such as personal stories. It is not scientifically reliable. Focus on information supported by scientific evidence and clinical studies. The quality levels of evidence from highest to lowest for medical data are:
- Systematic reviews: collect and evaluate all available data/evidence within the researchers’ criteria. An example is the “Cochrane Database of Systematic Reviews”. Meta studies are a systematic review.
- Randomized controlled trials: participants are randomly assigned to experimental and control arms. The double-blind trial is the gold-standard of medical research where neither the participants nor the researchers know the placebo or medication/treatment is given. This is to prevent bias and to ensure the validity and reliability of the study.
- Cohort observational study: participants with common traits or exposure to the proposed medications or treatments are followed over a long period of time.
- Case study or report: a detailed report of result after treatment of an individual. This is formalized and reviewed anecdotal evidence.
Medical Trial Reports
The phases of medical trial studies cited by published medical papers are:
- Pre-clinical studies: laboratory experiments using cell cultures, animal or computer models. In vitro means tested In Vitro – literally ‘in glass’ means testing outside a living organism, in a test tube or petri dish, In Vivo – literally in life -means testing in a living organism, often mice. Then studies move on to humans…
- Phase I trials: assess safety, dosage and side effects of the proposed medications or treatment.
- Phase II trials: expand P 1 to evaluate efficacy of the proposed medications or treatment – how well it works..
- Phase III trials: confirm efficacy, safety, dosage and to evaluate side effects of the proposed medications or treatment in much larger samples. This is often where randomized blind and double blind design is used. Blind means the patient does not know what they are getting; double blind means neither the patient nor the clinician know what is being dosed.
- Phase IV trials: monitor long term effectiveness and safety of the medication or treatment.
Statistical Terms
Some terms regarding statistical data cited in medical journals are explained as follows:
- N = the number of participants: be wary of studies with a very low N.
- HR = hazard ratio: HR=1 – there is no change in the proposed medication/treatment compared to control baseline. HR<1 – there is a reduction of risks with the proposed medication/treatment. HR>1 – there is an increase risk with the proposed medication/treatment.
- CI = Confidence Interval: A trial shows that a particular drug has a 20% effect within a certain time frame with 95% CI. This shows that the study, if repeated many times, it will be 95% confident that the 20% reduction will be consistently observed.
- P-value = Probability Value: This measures how strong the evidence is that the hypothesis, or effect being tested, is correct, rather than the result being random, or incorrect (null hypothesis). We seek a P-value that is <=0.05 meaning that there is a 95% or better likelihood the result is attributable to what is being tested..
Editor: Advisory Board Member and The Active Surveillor, Howard Wolinsky reminded us of another presentation AnCan presented a few years back A Layperson’s Guide to Reading Medical Research – watch it!
by CyberOptik | Oct 21, 2023 | Advocacy, Health Resources, Multiple Sclerosis, Veterans
So, you have MS. You may also be a Veteran of the United States military. What kinds of benefits and resources are available to those who have served and are now living with this debilitating disease? Here we hope you’ll find our beginner’s guide helpful in your search for benefits and resources.
Having MS and navigating the world of healthcare is dangerously daunting all on its own. Throw in some confusion about VA benefits, and you have a confusion cocktail to contend with (see what I did there?).
Before we dive in, just be warned: there is a plethora of information. Take your time researching, because there are a lot of links in this blog post. Because there’s so much info to take into consideration, we will do our best to update this blog as necessary. Check back regularly for more information as we come across it.
We have to thank Captain James “Jim” Marshall, who is a retired US Air Force Veteran, for bringing up this topic in the first place. Jim regularly moderates our Veteran Support Group, and also attends the High -Risk Prostate Cancer group & Blood Cancer group.
Over this past weekend, Jim struck up a conversation with an Air Force Veteran who has MS. He was surprised to learn that MS is, in fact, not covered under the Agent Orange Act or the PACT Act. MS has not been identified as an illness associated with the substances that these Acts target.
In his conversation, and subsequent research later on, he found that many people (perhaps as high as 60% of people) were denied upgrades to their disability rating. The VA, depending on evidence, will often award up to 30%. However, sometimes specific symptoms will allow for a higher percentage; one of those being chronic fatigue, which gets a 60% rating all on its own.
Jim also states that Veterans who are prevented from working as a result of their MS may be able to receive a benefit called
“Total Disability on Individual Unemployment Ability”, or TDIU. This benefit
compensates Veterans at the 100 percent rating, even if their overall disability rating may be less than that. Veteran’s symptoms must be Service-Connected (SC), and already have a 60% disability rating OR have “2 or more service-connected disabilities—with at least 1 rated at 40% or more disabling and a combined rating of 70% or more”. You also must not be able to hold down a steady job that would have supported you financially. Definitely click on he link above to read more about it and see if you qualify.
The website states: “The VA provides health care services to Veterans with MS from the time of diagnosis throughout their life, whether or not they have a service-connected or non-service connected status. If an individual had symptoms of MS in the military, or within seven years after honorable discharge, he/she may be eligible for service-connected disability.”
For those who are new to the benefits game:
The website suggests filling out the
VA Compensation and/or the
VA Pension form available online or at his/her local medical center for starters.
But oh my goodness, that’s a lot to sift through. Here are a few things on that web page that stand out to us:
Info on Filing and Intent to File – Sounds a little silly, but you may be able to receive retroactive payments for the time between when you submitted your intent to file and when they approve your claim.
Pension Benefit details – At least one of these must be true:
- You’re at least 65 years old, or
- You have a permanent and total disability, or
- You’re a patient in a nursing home for long-term care because of a disability, or
- You’re getting Social Security Disability Insurance or Supplemental Security Income
There’s more to this list, so click that link for info on Pension Benefits
Disability Housing Grants Information –
- Specially Adapted Housing Grant (SAH) for those who own their home, or will own their home, this is a grant that allows adaptive modifications to your home. Can receive up to $109,986 as of 2023
- Special Home Adaptation Grant (SHA) is the same as the above, but with different qualifications. Can receive up to $22,036 as of 2023
- Temporary Residence Adaptation for those who are living in a temporary family member’s home that needs changes in order to meet your adaptive needs. You must meet all the qualifying criteria for one of the two grants above. The amount changes depending on which one you qualify for.
Many people with a chronic or debilitating illnesses will tell you that advocating for yourself and your needs is of utmost importance. When dealing with and anything VA-related, persistence is key.
It’s tricky, and it’s a lot to deal with on top of managing symptoms.
Keep in touch with your primary care provider and your MS social worker. They’ll be able to help you refine your case for increasing your disability rating. They’re an invaluable source of information and help in signing up for various benefits. The provide supportive counseling to assist Veterans on the physical and emotional impact that MS can have on you and you family. They’re there to be your advocate, your negotiator, your case manager, and more.
If you don’t have a social worker on your team,
look for the Social Work department at your local VA, or talk to your primary care provider or MS Specialist.Here’s a summarized list of just some benefits offered at the VA. These programs require the help of a social worker:
Veteran Directed Care – offers monetary help with personal care services and daily living. Veterans are given a budget, and can even hire their own workers.
Medical Foster Home – This is a residency that’s similar to a nursing home, except Veterans are housed in a private home. Caregiving staff is on call 24/7. The VA ensures that these staff are well trained.
Other good Veterans Service Organizations (VSO) resources are:
Captain James “Jim” Marshall wants you all to know that if you have any questions pertaining to benefits and navigating the system, feel free to send him an email:
Marshall-James@comcast.net
As we mentioned above, this article is just a small portion of info about benefits in the VA system. We will continue to update or even create new blogs as we see fit.
Above all we sincerely thank each of our Veterans for their service. We love and appreciate you!
Don’t forget to check out our MS Peer Support Group, which meets every 2nd and 4th Tuesday of the month
And of course our Veterans Peer Support Group, which meets every 4th Thursday of every month
UPDATE #1 – Jim let me know that Amyotrophic Lateral Sclerosis (ALS) “is a presumptive condition for veterans with 90 days or more of continuously active service in the military. Any veteran with ALS should apply for Disability Compensation.”.
He goes on the state “Looking into justifying MS [and ALS] as Service-Connected, it is not as difficult as it seems. If the Vet was exposed to Hazardous Materials, most of us come across such things even in the states, then present VA thinking has MS service-connected because ‘IT IS AS LIKELY AS NOT’ caused by the exposure.”
