(Here is my take on this article Therapeutic Use of Cannabis and Cannabinoids A Review JAMA Network, 11/26/25. On a personal side, I use CBD to help me sleep, and with a little (5%) addition of THC, it is a great anxiety calmer – Sally Torgeson, AnCan Blood Cancer Moderator & Multiple Myeloma Coach)
Unapproved Cannabis
The FDA has NOT approved the cannabis plant (botanical marijuana) for any medical use or indication.
Because it is classified as a Schedule I controlled substance under federal law, the FDA has not found it to be safe or effective for the treatment of any disease or condition [1.1, 1.7].
It is currently illegal to market CBD by adding it to food or labeling it as a dietary supplement in interstate commerce [2.1, 2.5].
FDA-Approved Cannabinoid Drugs
The FDA has approved a small number of prescription drugs containing either a purified cannabis-derived compound or synthetic cannabinoids:
Epidiolex (Cannabidiol or CBD): The only FDA-approved drug that contains a purified substance derived directly from the cannabis plant. It is approved to treat seizures associated with Lennox-Gastaut syndrome, Dravet syndrome, and Tuberous Sclerosis Complex in patients one year of age and older [1.8, 2.1].
Marinol and Syndros (Dronabinol): Contain synthetic Δ9-tetrahydrocannabinol (THC). Approved for:
Nausea and vomiting associated with cancer chemotherapy in patients who have not responded to conventional antiemetic treatments [2.2, 2.3].
Anorexia associated with weight loss in patients with HIV/AIDS [2.3].
Cesamet (Nabilone): Contains a synthetic substance that is chemically similar to THC. Approved for chemotherapy-induced nausea and vomiting [1.1, 2.3].
Regulatory Context
The FDA maintains its authority to regulate products containing cannabis or cannabis-derived compounds, even those derived from hemp (cannabis with less than 0.3% THC), under the Federal Food, Drug, and Cosmetic (FD&C) Act [1.4].
The FDA supports the development of new drugs through proper clinical trials to ensure they meet standards for safety and effectiveness [1.1, 2.4].
FDA-Approved Cannabinoid Drugs and Their Conditions
* Nausea and vomiting caused by cancer chemotherapy (when other antiemetics have failed) * Anorexia (loss of appetite) associated with weight loss in patients with HIV/AIDS
Cesamet (Nabilone)
Synthetic cannabinoid (similar to THC)
* Nausea and vomiting caused by cancer chemotherapy (when other antiemetics have failed)
Key Takeaway
Epidiolex is the only drug approved that contains a substance derived directly from the Cannabis plant (CBD). It represents the strongest evidence for cannabinoid efficacy in reducing seizure frequency in certain rare forms of epilepsy [1.1, 1.2].
The synthetic THC compounds (Dronabinol and Nabilone) are used primarily as a last resort for severe nausea/vomiting related to chemotherapy and for appetite stimulation in AIDS patients [1.2, 2.8].
The FDA has not approved the use of the whole cannabis plant for any medical condition, stressing the importance of standardized, tested pharmaceuticals for patient safety and proven effectiveness [1.7].1
Off-Label Use vs. Unapproved Use
1. Off-Label Use (Legal and Regulated)
This applies only to drugs that the FDA has already approved.
What it is: Using an FDA-approved drug (like Epidiolex, Marinol, or Cesamet) for a condition, dose, or patient population that is not specifically listed on the drug’s official label.
Legality: It is legal for a licensed physician to prescribe an approved drug for an off-label use if they believe it is medically appropriate for their patient.
FDA Position: The FDA does not regulate the practice of medicine; however, the manufacturer cannot market or promote the drug for the off-label use. The safety and efficacy for the off-label use have not been verified by the FDA’s rigorous testing process.
Example: A doctor prescribing Marinol (Dronabinol), which is approved for nausea from chemotherapy, to a patient for chronic pain. The drug is approved, but the condition (chronic pain) is not on the label.
2. Unapproved Use (Non-FDA Approved Products)
This applies to the cannabis plant itself and most CBD/cannabinoid products on the market.
What it is: Using the whole cannabis plant (botanical marijuana) or non-FDA-approved cannabis-derived products (like most CBD oils, edibles, or topicals) for any medical purpose.
Legality:
Federal: The whole plant is a Schedule I controlled substance and is not federally approved for any medical use.
State: Use may be legal under state medical or recreational cannabis laws, but this does not change its status as an unapproved drug under federal FDA law.
FDA Position: The FDA considers these products unapproved drugs and/or illegally marketed products (especially when CBD is added to food or marketed as a dietary supplement), as they have not been tested for safety, effectiveness, or quality assurance.
Example: A patient using a CBD tincture (which is not Epidiolex) to treat anxiety, or using THC flower to help with multiple sclerosis symptoms.
To correspond with Sally, please send an email to info@ancan.org, and we’ll be sure to send along.
Has eating become a challenge due to fatigue or a lack of interest in food? Have you noticed a significant change in your or your loved one’s appearance since starting treatment or diagnosis?
It’s a common misconception that weight loss during cancer treatment is solely due to treatment side effects. While this can certainly be a factor, a more serious condition known as cachexia (kuh·kek·see·uh) can significantly impact a patient’s health.
What is Cachexia and Who is at Risk?
Cachexia, often referred to as cancer cachexia or wasting syndrome, is a complex condition characterized by severe weight loss, muscle wasting, and loss of appetite. It’s not a direct side effect of cancer treatment but rather a consequence of the cancer itself. While it’s commonly associated with cancer, it’s important to note that cachexia can affect individuals with various chronic illnesses, including: Multiple Sclerosis, Sarcoidosis, heart failure, chronic kidney disease, COPD, and more. Certain types of cancer are more likely to lead to cachexia than others. These include: Pancreatic, Lung, Head and Neck, Colorectal, Ovarian, and Liver.
Signs and Symptoms of Cachexia: What Should You Look For?
Recognizing the signs of cachexia is crucial for early intervention and effective management. Here are some key symptoms to watch for:
Unexplained weight loss: A significant and unintentional decrease in weight.
Muscle loss: A noticeable loss of muscle mass, often leading to weakness and fatigue.
Decreased appetite: A reduced desire to eat, even when hungry.
Fatigue: Persistent tiredness and a lack of energy.
Metabolic changes: Alterations in metabolism, including changes in appetite, weight, and energy levels.
Changes in Routine: Unable to do the activities you once could.
If you or a loved one is experiencing these symptoms, it’s important to let your care team know your concerns as soon as possible.
Managing Cachexia
While there’s no one-size-fits-all solution, a multidisciplinary approach can help manage the condition. This may involve:
Dietary interventions: A registered dietitian can provide personalized meal plans to maximize nutrient intake.
Medical treatments: In some cases, medications may be prescribed to stimulate appetite or reduce inflammation.
Supportive care: This includes strategies to manage pain, fatigue, and other symptoms.
Psychological support: Counseling can help address emotional challenges associated with cachexia.
This may mean adding more people to your careteam to support you, such as a dietician (as shown above), physical or occupational therapist, endocrinologist, or palliative care (editors note: we hope you already have a palliative care doctor, AnCan loves them and they can offer you so much support during your treatment!)
Coping with the Emotional Impact
Cachexia can take a significant toll on both physical and emotional well-being for the patient, care-partner, and their families. It’s important to seek support to manage the emotional side effects of the condition. Consider:
Counseling: Individual, couples, or family therapy can provide guidance and coping strategies.
You can also ask your social worker (or for a social worker if you do not have one) for additional resources.
Want to Learn More?
We highly recommend this webpage and fact sheet from our friends at Cancer Support Community / Gilda’s Club. While it is cancer centric, all of the information will be of helpful no matter what your diagnosis is.
By understanding the complexities of cachexia and seeking appropriate support, individuals can significantly improve their quality of life. Effective management of cachexia can help alleviate debilitating symptoms, enhance overall well-being, and improve the ability to participate in daily activities.
Special thanks to CSC for their assistance and incredible resources with this blog post.
A couple of weeks back, we posted Medicare Health Insurance Choices that explained the differences and pitfalls between traditional Medicare Part A and B plus Medigap insurance plans to Part C, Medicare Advantage. Click the link earlier in the previous sentence if you missed it.
As many already know, there is a Part D that covers drug costs. It is either purchased as a separate plan or rolled into Part C Advantage. Drug coverage is significantly changing this year, and AnCan has learnt that many of our participants are not yet aware. Hardly surprising because CMS as well as the various stakeholders like Payers and providers have done very little to let us patients know. Why should they? – we’re only the ultimate consumer!
The same cannot be said of JnJ who started educating patient advocate organizations this past May. In October and November JnJ created more education that includes a webinar and a round table coming up hosted by NAMAPA, the National Association for Medication Access and Patient Advocacy. Likely you have never heard of them. I hadn’t and it hardly rolls off the tongue. Nonetheless, the webinar was very instructive and you can watch it here.
The BIG difference for us patients is that no matter what, out-of-pocket drug costs for 2025 cannot exceed $2000. You heard right – for those of you on specialty oral medications like Nubeqa (darolutamide for prostate cancer) or Aubagio (teriflunomide for MS), normally sourced via specialty pharmacies, you will meet this cap January. And you’ll even be able to spread the payment over 12 months! More on that to follow.
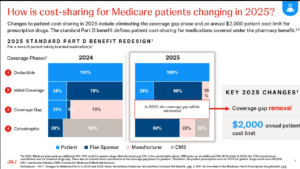
But first, how is this coming about. Well it tracks back tot he changes brought about by the Inflation Reduction Act signed by President Biden in 2022. He promised to make drugs more affordable, and this is a part of the plan. As you can see in the slide to the left comparing 2024 to 2025, the donut hole has been eliminated. In its place, the Payer (Plan Sponsor) and Pharma (manufacturer) are paying more. While the cost saving is very positive, it will likely impact us patients in other ways:
Your formulary choice may be reduced – so CHECK your medications before you renew.
Premiums for Part D may increase – even though out of pocket is capped. If you are unlikely to spend $2,000, look for a plan that defers your co-pay as long as possible
Higher premium plans should cover a larger portion of drug costs earlier. Your premium does NOT count towards the $2,000, so include premiums in your cost calculation to figure your exposure.
If you have a co-pay or co-insurance on your drugs, no matter if it’s Part C or D, it cannot exceed $2,000. However the amount you pay and who you pay it to may become a bit of a moving target. We mentioned earlier that you will now have the opportunity to spread your payments over the calendar year – or the remainder of it, if you sign up late or incur costs late in the year. The Medicare Prescription Payment Plan (M3P) takes your share of drug costs, up to a maximum of $2,000, and spreads them over the remainder of the year.
The simple example is for those on specialty pharmaceutical drugs like Nubeqa or Aubagio. Since your share of the drug cost is almost certainly going to be greater than $2,000 in January, if you opt in for M3P BEFORE going to the pharmacy or ordering from your mail order pharmacy, you’ll pay nothing on picking up/shipping the drugs. Subsequently, you’ll get a separate bill from your Payer for $167.67 monthly over 12 months, and pay no more for any of your drugs the rest of the year. There is NO interest, no late fee penalties, and you get a couple of months leeway, but there are penalties if you never pay. You can sign up for MP3 with your Medicare Payer/Plan Holder BUT not in the pharmacy for 2025. So if you arrive at the drug store prior to enrollment, you’ll be charged $2,000 to take your pills home. You can leave the pills, go home, enroll and return to the pharmacy 24 hours later and pick up without payment to the pharmacy..
If you don’t start this expensive drug until mid year, say September, and you’ve spent nothing on drugs prior, then the $2,000 is billed over the last 4 months at $500/month.
But what if your drug costs are more lumpy – they go up and down the whole year. In that case, the payments get recalculated each month and the monthly bill will vary.
There is a strange case too, if you know your co-pay is the same each month – say $55. This really throws M3P, and as you can see to the left, you’ll pay the same $660 (12x $55) either way but in different amounts each month if enrolled in M3P.
Finally, let’s address the Drug Benefit plans that many of you enjoy through PAN, PAF and others. Even the drug discount cards from Pharma that some receive. Whatever you receive, or however you receive it, does NOT reduce your $2,000 exposure. You advise the pharmacy that you have a benefit, and they bill the Benefit Provider (PAN, PAF, Pharma ??). The credit will be applied against your drug cost, although eventually you may still be liable for up to $2,000 co-pay when the benefit runs out.
Looking at the first slide, it seems to AnCan that these benefits that are often funded by Pharma, eventually flow back to Pharma and the Payer. How they will credit them against what the patient owes is not yet clear. Before you get too crazed, our guess is the system has to change. These benefits need to be channeled directly to patients who cannot afford $2,000 p.a. AnCan is on it and already reaching out to NAMAPA and others to promote more of a direct, income based subsidy possibly reaching more beneficiaries. One thing we have heard – APPLY EARLY for 2025 in the event you are in line to receive a subsidy.
PLEASE BE SURE TO SIGN UP FOR THE M3P PROGRAM UPFRONT. EVEN IF YOU OWE $2,000 IT WILL BE BILLED IN 12 INSTALLMENTS. WE STILLL HAVE TO FIGURE HOW YOU WILL BE REIMBURSED IF YOU RECEIVE ASSISTANCE.
IF YOU HAVE A GRANT BE SURE TO PROVIDE DETALS TO THE PHARMACY ASAP. NOTWITHSTANDING, ALSO REACH OUT TO YOUR GRANTOR TO FIND HOW THEY WANT TO COORDINATE THE GRANT. IT’S STILLL A MOVING TARGET!
This could be scary…It’s almost open enrollment season for Medicare!
A dreaded time to receive multiple communications in untold ways that often read like a foreign language. It’s only fitting that we talked about it the day before Halloween.
Join AnCan as we bring experts Amanda Goodstadt, Esq. from Triage Cancer, and Medicare Insurance Broker Kim Umphres to explain all things confusing around 2024 Medicare insurance options, and make this enrollment season a little less spooky and intimidating.
Our panel will explain the whole menu from alphabet soup plans to doughnut holes! Learn the difference between Traditional and Advantage plans and if you can switch between them, what HMOs and PPOs mean, how to sign up to see any doctor anywhere and much more.
Click here for a special handout from Triage Cancer with Medicare resources.
Special thanks to Bayer, Pfizer, Myovant Sciences, Foundation Medicine, Myriad Genetics, Janssen – Johnson & Johnson, Telix, and Blue Earth Diagnostics for sponsoring this webinar.
To SIGN UP for any of our Virtual Support groups, visit our Contact Us page.
AnCan Foundation supports several conditions that compromise the pelvic floor as a result of surgery, radiation, or just side effects of the disease itself. It can impact continence and sexual function for all!
A non-interventional rehab solution is pelvic floor physical therapy – a sub-specialty in itself.
Join one of AnCan’s favorite superstars, urologist Dr. Rachel Rubin, and esteemed expert Dr. Tracy Sher. Together, shared how pelvic floor exercises can help you recover function!
You’ll also get a ton of questions answered, asked by MS Moderator Kim Stroeh, and Prostate Cancer moderator Dr. John Antonucci.
Watch here:
Special thanks to Bayer, Pfizer, Myovant Sciences, Foundation Medicine, Myriad Genetics, Janssen – Johnson & Johnson, and Telix for sponsoring this webinar.
Check back later for slides.
For information on our peer-led video chat VIRTUAL SUPPORT GROUPS, click here.
To SIGN UP for any of our Virtual Support groups, visit our Contact Us page.

 Off-Label Use vs. Unapproved Use
Off-Label Use vs. Unapproved Use
 and this is a part of the plan. As you can see in the slide to the left comparing 2024 to 2025, the donut hole has been eliminated. In its place, the Payer (Plan Sponsor) and Pharma (manufacturer) are paying more. While the cost saving is very positive, it will likely impact us patients in other ways:
and this is a part of the plan. As you can see in the slide to the left comparing 2024 to 2025, the donut hole has been eliminated. In its place, the Payer (Plan Sponsor) and Pharma (manufacturer) are paying more. While the cost saving is very positive, it will likely impact us patients in other ways: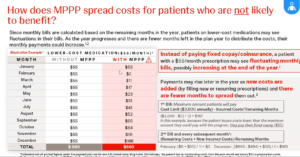 But what if your drug costs are more lumpy – they go up and down the whole year. In that case, the payments get recalculated each month and the monthly bill will vary.
But what if your drug costs are more lumpy – they go up and down the whole year. In that case, the payments get recalculated each month and the monthly bill will vary.