Taking on the role of a care partner can feel overwhelming, but you don’t have to navigate it alone. Many experienced care partners will tell you that with a little guidance, it can also be a deeply fulfilling experience. To help you on your journey, we’ve compiled some helpful resources available online.
1.Leaning Into Grief: An Interview With Claire Bidwell Smith
Claire Bidwell Smith is a therapist, grief expert, and author. Click here for her interview about leaning into grief.
2. Cancer Today: Addressing Anger
Anger and Irritability are normal responses to a cancer diagnosis, and this article offers guidance for care partners of cancer patients.
3. NCCN Guidelines for Patients: Palliative Care
The National Comprehensive Cancer Network released an easy to read, patient-centric Palliative Care guidelines that you can view and download. Click here.
4. “Caregiver Life Hacks”
There’s no one-size-fits-all way to care for someone because every care partner and situation is different. What helps one person might not work for another, but many care partners deal with similar challenges. Click here for some simple “life hacks” that might make your day a little easier.
5. “Caregivers Need Care Too”
“However, primary care partners are also thrust into an unfamiliar world of medical treatments, terminology, and appointments. This is why mutual support between the patient and the primary care partner is important—it is a partnership through thick and thin because both the patient and primary care partner need to learn about the complexities of the disease and treatments needed, as well as make important decisions together.” Click here for the full article.
6. Triage Health Caregiver Resources
Click here for a full list of resources about legal and practical matters like taking time off from work, managing family finances and medical bills, replacing lost wages, estate planning, and other resources.
7. Cancer Straight Talk Podcast: Advice and Support for Cancer Caregivers
The podcast Cancer Straight Talk features host Dr. Diane Reidy-Lagunes speaking with Dr. Allison Applebaum, the founder of the Caregivers Clinic at Memorial Sloan Kettering Cancer Center (MSK). This episode covers navigating the healthcare system and managing the emotions of caregiving.
8. Patient Power: Power of Care Partners: Who Has your Back?
This article is about the crucial role of care partners for people with chronic illness. It distinguishes a “care partner” as a full member of the care team, not just a caregiver. The article also provides advice on practical matters, like having a designated care partner with access to medical records, and emphasizes the importance of care partners looking after their own well-being.
Tomorrow is the 10th Anniversary of my dear friend, Jerry Carniglia’s passing, God Rest His Soul.
I loved this man. I found him in 2011, when my buddy Eric Schmier GRHS/z”l asked me to navigate him. That’s the same Schmier after whom we named one of our Virtual Room when his family made a very generous donation early in AnCan’s history. Jerry had been diagnosed with denovo metastatic prostate cancer and was being treated inadequately at Kaiser Permanente in Oakland, CA.
Eric was a developer in Emeryville, Caifornia, and Jerry was the ‘unofficial’ Mayor. Everybody knew him – he lived in a disused 6,000 s.f. factory turned into his living space and studio. Jerry was a general contractor, artisan woodworker with an enormous, fully equipped workshop, an artist of very large (& small) canvasses, and not least an actor. Jerry’s closest buddy from drama school at UC Berkeley school was Tony award winner, Tony Taccone, Artisitic Director at Berkeley Rep. You may be familiar with Tony’s son and Jerry’s Godson, Jorma Taccone of Lonely Island and Saturday Night Live fame (Dick in the Box).
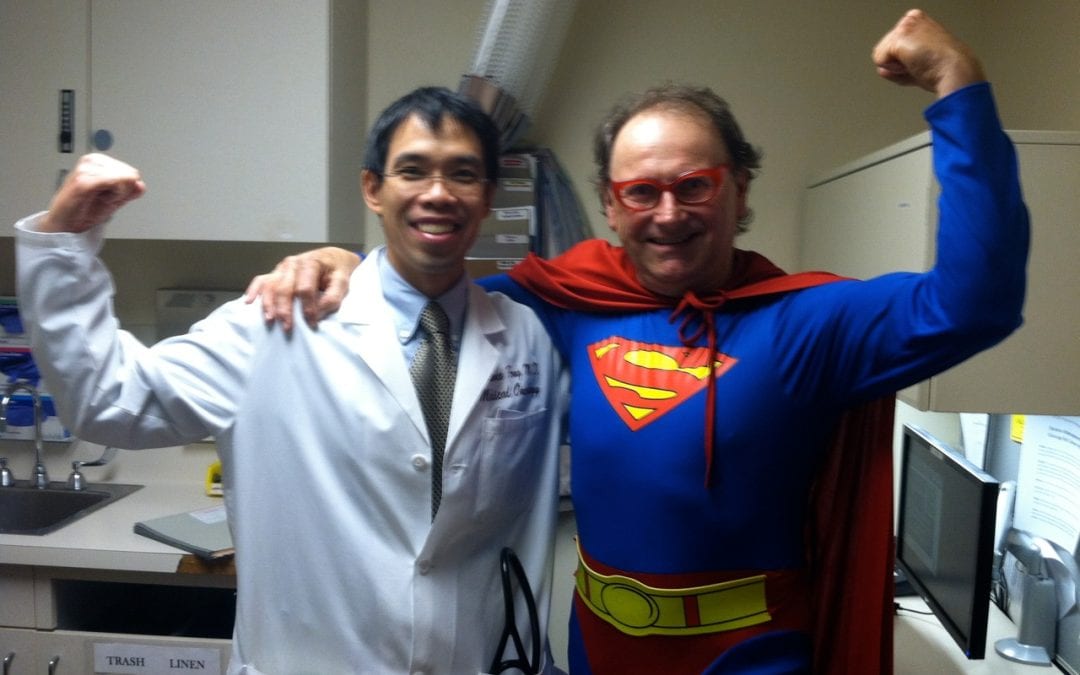
Jerry was diagnosed with denovo metastatic prostate cancer in 2011, and we transferred his care from KP to UCSF as soon as we could under the amazing, watchful eye of Dr. Larry Fong. Larry is the Principle Investigator for Provenge and a highly respected GU medical oncologist. Jer’s prognosis was not great and we got him around 4 years.
This picture was taken on Halloween 2012 on the occasion of Jerry receiving his 3rd Provenge infusion!
Amongst other pre-‘AnCan’ directed navigation, Jerry was the first Veteran I supported. When I discovered he’d served on a Blue Water craft in the Mekong Delta. we got him over $4 Grand a month! And it was through Jerry that AnCan found our Care Partner Lead Susan Lahaie, and her late husband, Ron Silverio.
Jerry decided he wanted to document his last years. He bought a fancy camera, the softtware program First Cut that he taught himself, and started making videos. It did not hurt that he had many connections to assist him with video, audio, editing and production. In Jerry’s dear memory, I want to bring several videos to your attention that are now lodged on You Tube. You’ll find me reluctanty appearing in two of them!
Jerry Carniglia, Painter is a short video displaying his remarkable technique. I suspect, although I’m not certain, this canvas may be one of the 3 Carnigloa paintings I have hanging in my casita. Much of his work was donated to UCSF and to Larry Fong personally. He is collectable and had several shows.
Jerry Cut 3 – is an edited collage of several clips Jerry made in his own memory. He intended them to be watched as you are doing today This is Jer!!
Painting A Quiet Radical, a 5 min short, is scripted and acted by Jerry and friends who also lived with advanced prostate cancer. Other than myself, the other’s are no longer with us. His Tony award winning director friend, Tony Taccone refused to have any part of this, then showed up at the read-through and directed the whole 9-yards!
Signs is the re-enactment of a true event when Jerry went for an evening stroll along the railroad tracks close to his factory, He tripped, fell, knocked himself out and almost got run over by a train. I tracked him down several days later in the hospital. A few months later Jerry called me up one Monday morning in the Fall and told me to come by that afternoon. We were filming! I asked what – and where’s the script. He said – “Just show up wearing shorts and sandals. You don’t need a script!” Gotta love this man.
This post is a tribute to Jerry Lee Carniglia. He died on June 7, 2015 – may his memory always be a blessing. It will to me.
“Someone I once loved gave me a box of darkness” –Mary Oliver
I was at a 12-Step-oriented workshop about grief recently, and it made me think about Men Speaking Freely (MSF). We are vaguely aware of grief in all MSF groups, it hangs over us, and we have at times focused on some specific griefs/losses, such as vitality, or a longer life. It is commonly thought that not thinking about a loss, not talking about it is the manly thing to do. Here in MSF we get relief by sharing our common losses with each other.
The presenter of that workshop, Marcia C., had some ways to specifically talk about grief that were new to me. She gave me permission to use some of her material here. She pointed out some types of losses that I hadn’t realized. For example, the loss of who I would have been if cancer didn’t happen, the grief of estrangement, loss of work, of status, of friendship; the loss of never having had something, that of aging, of trust, or of giving up something.
She said there is “unacknowledged grief” when such losses are never fully brought to consciousness. When I looked at her long list of examples I saw many that I have. We ought to watch for unacknowledged grief.
She described “non-finite” grief, which has no end-point other than death. Ours could be in that category, since as time goes by our loss increases instead of lessens.
Marcia said, ‘’Sharing your grief is a way to receive validation and compassionate witnessing. It can help you begin a path to healing and/or finding a way to live with grief.
Consider the questions below:
1. Are there griefs you haven’t realized you have or have been afraid to face?
2. Are there griefs about which you’d like to share?
3. Do you have grief practices that might be helpful to others?
4. Make a list of griefs you’ve experienced.
5. Choose a tool from the list that might help you process your grief.”
That list of “tools” was long; it included things like: write a letter or poem describing our loss…Create a ritual of letting go…Share with others who have had similar losses…Visit a place that is meaningful…Make or buy a talisman that helps you feel protected…Dance, run, yell to get your feelings out of your body…Plant something in remembrance or as a new beginning…Start a new tradition…Do an intentional funeral… These are ways to bring acknowledged, unacknowledged, and non-finite grief out for a conscious conversation. Moving from covert to overt, with the goal of making a relationship with the loss, and getting rid of the unconscious silent prolonged scream that I, for example, think I harbor.
We think of grief as emotional, but in “Dealing With the Physical Impact of Intense Grief” by Batya Swift Yasgur, the author describes the variety of physical reactions to grief. Ranging from elevated blood pressure to takotsubo cardiomyopathy — sometimes called “broken heart syndrome” — which is a “stress response that balloons the heart.” We often wonder about the reaction on our immune system, and its implications to our overall survival. In fact, probably nearly all our systems react to grief in some way.
There is a fairly new grief-related diagnosis in the Diagnostic and Statistical Manual and the International Classification of Diseases, describing a “persistent and pervasive grief response” that goes on longer than a year., and is now called Prolonged Grief Disorder. In order to be diagnosed with Prolonged Grief Disorder, a person must experience at least three of eight additional symptoms that include “disbelief, intense emotional pain, feeling of identity confusion, avoidance of reminders of the loss, feelings of numbness, intense loneliness, meaninglessness, or difficulty engaging in ongoing life” according to Columbia University’s Center for Prolonged Grief. For an adult to meet the criteria for a PGD diagnosis, the death of a loved one must have occurred at least one year ago, and the symptoms must be present most days since the loss and nearly every day for at least the last month.
Our situation is different from losing a loved one (although it includes that) and waiting for the grief to go away. Instead of a major loss which goes farther and farther into the past, our major loss is in the future. We have sort of a reverse Prolonged Grief Disorder. For instance, I expect my losses to get worse and worse until death.
Has eating become a challenge due to fatigue or a lack of interest in food? Have you noticed a significant change in your or your loved one’s appearance since starting treatment or diagnosis?
It’s a common misconception that weight loss during cancer treatment is solely due to treatment side effects. While this can certainly be a factor, a more serious condition known as cachexia (kuh·kek·see·uh) can significantly impact a patient’s health.
What is Cachexia and Who is at Risk?
Cachexia, often referred to as cancer cachexia or wasting syndrome, is a complex condition characterized by severe weight loss, muscle wasting, and loss of appetite. It’s not a direct side effect of cancer treatment but rather a consequence of the cancer itself. While it’s commonly associated with cancer, it’s important to note that cachexia can affect individuals with various chronic illnesses, including: Multiple Sclerosis, Sarcoidosis, heart failure, chronic kidney disease, COPD, and more. Certain types of cancer are more likely to lead to cachexia than others. These include: Pancreatic, Lung, Head and Neck, Colorectal, Ovarian, and Liver.
Signs and Symptoms of Cachexia: What Should You Look For?
Recognizing the signs of cachexia is crucial for early intervention and effective management. Here are some key symptoms to watch for:
Unexplained weight loss: A significant and unintentional decrease in weight.
Muscle loss: A noticeable loss of muscle mass, often leading to weakness and fatigue.
Decreased appetite: A reduced desire to eat, even when hungry.
Fatigue: Persistent tiredness and a lack of energy.
Metabolic changes: Alterations in metabolism, including changes in appetite, weight, and energy levels.
Changes in Routine: Unable to do the activities you once could.
If you or a loved one is experiencing these symptoms, it’s important to let your care team know your concerns as soon as possible.
Managing Cachexia
While there’s no one-size-fits-all solution, a multidisciplinary approach can help manage the condition. This may involve:
Dietary interventions: A registered dietitian can provide personalized meal plans to maximize nutrient intake.
Medical treatments: In some cases, medications may be prescribed to stimulate appetite or reduce inflammation.
Supportive care: This includes strategies to manage pain, fatigue, and other symptoms.
Psychological support: Counseling can help address emotional challenges associated with cachexia.
This may mean adding more people to your careteam to support you, such as a dietician (as shown above), physical or occupational therapist, endocrinologist, or palliative care (editors note: we hope you already have a palliative care doctor, AnCan loves them and they can offer you so much support during your treatment!)
Coping with the Emotional Impact
Cachexia can take a significant toll on both physical and emotional well-being for the patient, care-partner, and their families. It’s important to seek support to manage the emotional side effects of the condition. Consider:
Counseling: Individual, couples, or family therapy can provide guidance and coping strategies.
You can also ask your social worker (or for a social worker if you do not have one) for additional resources.
Want to Learn More?
We highly recommend this webpage and fact sheet from our friends at Cancer Support Community / Gilda’s Club. While it is cancer centric, all of the information will be of helpful no matter what your diagnosis is.
By understanding the complexities of cachexia and seeking appropriate support, individuals can significantly improve their quality of life. Effective management of cachexia can help alleviate debilitating symptoms, enhance overall well-being, and improve the ability to participate in daily activities.
Special thanks to CSC for their assistance and incredible resources with this blog post.
Last month’s Under 60 Stage 3 & 4 Prostate Cancer meeting was small, intimate and produced a true gem from Down Under to benefit all AnCan’rs …
For the life of me, I forget what raised the topic … maybe a Death with Dignity discussion – but Aussie AnCan’r, Steve Cavill told us about the ICE “In Case of Emergency” Checklist Document that he and his wife Leonie, who occasionally attends our Care Partners Group, have both completed. Steve and Leonie reside in the suburbs of Melbourne and are currently heading towards mid-Winter.
This ICE Checklist takes much, if not all, the difficulty out of placing your key information in one place. Like your vital passwords to your laptop, phone or bank accounts; names of key individuals in your life and more. You know .. all that information making it possible for someone to piece your life together if you’re suddenly no longer with us.
Frankly it’s information we should all compile no matter how old. With this checklist guide at hand to march us through it, there can be few excuses. Just remember, this version of the ICE checklist was created in Oz, so it may not be fully applicable Stateside. If one of our US volunteers has time to ‘Americanize’ it, I feel sure it will be greatly appreciated – we have very few solicitors in the US and a few too many attorneys!
Here’s the checklist document in Word format ICE Document Template Now do your part …. and a BIG THANK YOU, Steve Cavill!!
Hi-Risk/Recurrent/Advanced PCa Video Chat, May 15, 2023
AnCan is grateful to the following sponsors for making this recording posssible: Bayer, Foundation Medicine, Pfizer, Janssen, Myriad Gentics, Myovant & Telix
AnCan Foundation deeply mourns our dear Board & Advisory Board Member, Moderator and Brains Trust Brother, Herb Geller. To read more click https://mailchi.mp/ancan/remembering-…
All AnCan’s groups are free and drop-in … join us in person sometime! You can find out more about our 12 monthly prostate cancer meetings at https://ancan.org/prostate-cancer/ Sign up to receive a weekly Reminder/Newsletter for this Group or others at https://ancan.org/contact-us/
Editor’s Pick: Controversial Death with Dignity discussion starts – and Keytruda shows up more than once at the back end … after passing Dude Wipes along the way! (rd)
Topics Discussed
Talking ‘Death with Dignity’ with AnCan Advocate; urologist refuses Provenge – get a GU med onc!; pros & cons of treating the primary; timing of RT; handling multiple QBs; Bx find no NEC; salvage RT commenced; clean up with Dude Wipes; brain fog/short term memory loss – drug and non-drug remedies; Flomax and brain fog; some Gents take just 2.5mg/daily prednisone with abi; Eligard & ukuleles; another Gent looks to pembro/Keytruda; proteomics; wean off Prolia; pembro vs chemo decision
Chat Log
Ben Nathanson sent · 5:14 PM As the End Nears: Dying with Metastatic Cancer https://join.compassionandchoices.org/a/end-nears-dying-metastatic-cancer Compassion & Choices https://www.compassionandchoices.org States where medical aid in dying is authorized, and dates when it took effect: Oregon 10/27/1997 Washington 3/5/2009 Montana 12/31/2009 Vermont 5/20/2013 California 6/9/2016 Colorado 12/16/2016 Washington, D.C. 2/18/2017 Hawai‘i 1/1/2019 New Jersey 8/1/2019 Maine 9/19/2019 New Mexico 6/20/2021
Joe Comanda (Philadelphia) sent · 5:21 PM I don’t want to cause trouble, but I am troubled by the advocacy of Compassionate Choices, formerly the Hemlock Society. I would hope that men would not take that way out.
Len Sierra sent · 5:23 PM Everyone has to make that decision for themselves. No one else should make it for them.
rd sent · 5:24 PM We think it’ s each person to his own… AnCan believes everyone has a choice, Joe.
Jim B sent · 5:36 PM Hi Bob, I just had a Pluvicto treatment this morning. No side effects so far but I’m sure that dry mouth, nausea and slight fatigue will continue. How is your WBC coming along?
Joe Gallo sent · 5:47 PM Genito Urinary (GU) Oncologist Dr. Eleni Efstathiou
Peter K sent · 6:37 PM I have had 3 med oncs for over a year now. 2 up to a year ago. They are all valuable and I keep them all informed and they all have vaulable input
rd sent · 6:38 PM MDA – maybe the best cancer hospital … but not the best prostate cancer hospital
Peter K sent · 6:42 PM They are doing MRidian SBRT with View Rayt in Michigan- low toxicity in trials



 I loved this man. I found him in 2011, when my buddy Eric Schmier GRHS/z”l asked me to navigate him. That’s the same Schmier after whom we named one of our Virtual Room when his family made a very generous donation early in AnCan’s history. Jerry had been diagnosed with denovo metastatic prostate cancer and was being treated inadequately at Kaiser Permanente in Oakland, CA.
I loved this man. I found him in 2011, when my buddy Eric Schmier GRHS/z”l asked me to navigate him. That’s the same Schmier after whom we named one of our Virtual Room when his family made a very generous donation early in AnCan’s history. Jerry had been diagnosed with denovo metastatic prostate cancer and was being treated inadequately at Kaiser Permanente in Oakland, CA. Jerry was diagnosed with denovo metastatic prostate cancer in 2011, and we transferred his care from KP to UCSF as soon as we could under the amazing, watchful eye of Dr. Larry Fong. Larry is the Principle Investigator for Provenge and a highly respected GU medical oncologist. Jer’s prognosis was not great and we got him around 4 years.
Jerry was diagnosed with denovo metastatic prostate cancer in 2011, and we transferred his care from KP to UCSF as soon as we could under the amazing, watchful eye of Dr. Larry Fong. Larry is the Principle Investigator for Provenge and a highly respected GU medical oncologist. Jer’s prognosis was not great and we got him around 4 years.

